
Connexions : no.25(1987)
- Title
- Connexions : no.25(1987)
- Description
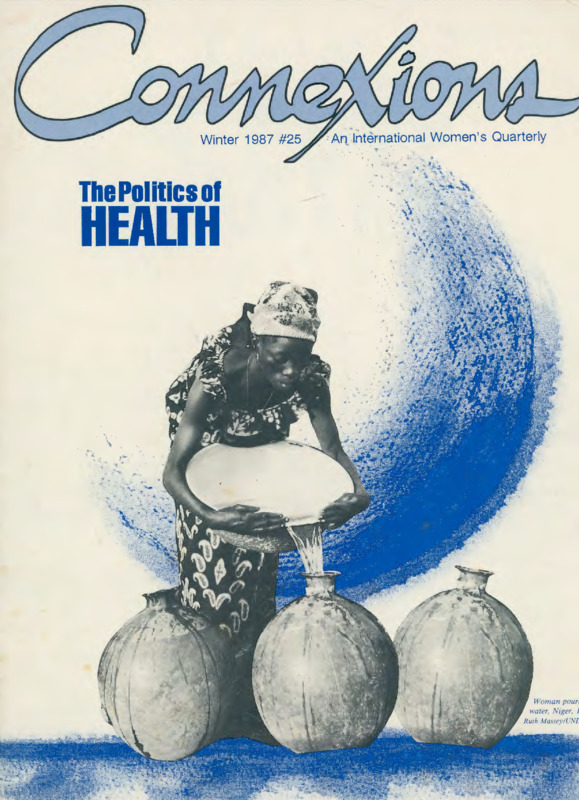
- Connexions is published by People’s Translation Service quarterly and each issue focuses on a unifying theme. The goal of Connexions is to provide a space for international women to contribute to one unified women’s movement. This issue of Connexions, published in winter of 1987, has a theme of the politics of health and includes poetry, a question and answer segment, and academic-style writing on topics such as involuntary sterilization, genital mutilation, access to water, and intersectionality.
- Date Issued
- 1987
- Relation
- Connexions
- Rights
- Contact UCO Chambers Library's Digital Initiatives Working Group at diwg@uco.edu for the permission policy on the use, reproduction or distribution of this material.
- Contributor
- People's Translation Service
- Date
- 2024-11-26T00:00:14Z
- Date Available
- 2024-11-26T00:00:14Z
- Subject
- Health
- extracted text
-
An_ International Women 's Quarterly
The Politics or
HEALTH
1 Introduction
2 India: Eliminate Inequality, Not Women
The abuse of amniocentesis may lead to female extermination.
4 Britain:
Robbed of Colour
Due to vitiligo, a Black woman is losing her color.
6 Senegal: Change the Mentality, Not the Skin Color
Black women are pressured to lighten their skin with dangerous compounds.
7 Britain: Fat Women Fight Back
Fat women fight societal standards of health and beauty.
8 Canada: Screaming in the Wind
A woman reports on her many years of experience in mental institutions.
10 West Germany: Sterile Without Consent
Disabled women are being involuntarily sterilized.
12 Update: Restricted "Choice"
Abortion rights updates from Ireland, Israel, India, Hong Kong, Mauritius and Japan.
15 Costa Rica: The International Meeting on Women and Health
Women exchange resources and information.
16 Nigeria: AIDS Linked to Genital Mutilation?
Hannah Edemikpong discusses a possible correlation between genital mutilation and AIDS in Africa.
18 India: Cooking Inside
The effect of wood smoke on the health of women.
20 Kenya: Water: An Obstacle for African Women
Women's water projects help to provide better quality drinking water and sanitation.
23 Canada: Woman and Substance Abuse
Women work together to fight substance abuse.
24 Collectives:
Together We Are Strong
Women organize for better health in Switzerland, Berlin, Bangladesh, Mauritius, and Nicaragua.
26 Shorts:
Health shorts from Malaysia, Canada, Switzerland and New Zealand.
29 Letters
30 Health Resources for
Women
Office Staff
Constantina Bertone, Linda Fogel, Shoshana Friedkin,
Pally Ruppel!, Anne-Marie Schmoltner, Donna Scism,
Patricia Sieber, Iris Wesselmann.
For This Issue
Editorial
Constantina Bertone (co-coordinator) , Amy Christiansen , Karen Hayashi , Leslie Jones, Viki Radden , AnneMarie Schmoltner, Donna Scism (co-coordinator),
Patricia Sieber, Janis Steele, Iris Wesselmann.
Production
Constantina Bertone (coordinator, typeselling), Dee
Elling (cover), Linda Harrold (proofreading), Leslie
Jones, Leslie Katz, Ellen Owens, Pally Ruppelt (typesetting), Donna Scism (typese11ing), Janis Steele, Iris
Wesselmann
Translation
Viki Radden (French), Anne-Marie Schmoltner (German), Donna Scism (Spanish), Patricia Sieber (German ,
French)
Special Thanks To:
Mark Manzione, Ines Rieder
Statement
Connexions is the collective product of feminists of
diverse nationalities and political perspectives committed to contributing to an international women's movement.
We want to go beyond merely providing facts
and information, and hope that by passing on-as
directly as possible-women's writing generally unavailable in the US, we will be helping women here to
understand and connect with the experiences and
viewpoints of women in other parts of the world. We
also want to contribute to the growth of a worldwide
network connecting women working on similar projects
by researching, establishing contacts and exchanging
information with other women 's organizations.
To a large extent, the economic and political
conditions under which we live determine the issues to
which we give priority. Women do not live in a
vacuum, but in what is still largely a man's world. It is
essential for us to understand the working of that world
if we are to understand each other. We hope that Connexions will be one step toward building an international women 's movement.
Connexions is a quarterl y and each issue focuses on a
specific theme. Connexions is published by People's Translation
Service. 4228 Telegraph A venue, Oakland. CA 94609. Subscription rates are $ I 2 per year: Canada and Mexico US$ I 4:
Overseas-US$ I 4 surface. US$20 airmail. An annual institu•
tional subscription is $24. Please send international money orders in US$ or international travelers' checks in US $.
Articles and photographs from Connexions may be
reprinted free of charge by non-profit publications without per~
mission except where accompanied by cop yright. (Others please
inquire for reprinting rights.) Please credit Connex ions. including
our subscription rates and address whene ver reprinting our
material. and please send us a tearsheet. Connexions is indexed
in th e Aliernati,·e Press Index, P.O. Box 7229. Baltimore. MD
2 1218.
ISSN 0886· 7062 .
The Politics
of HEALTH
SAMPL~ COPY
Who is concerned with women's health? Those who have power over
women's health issues often show little concern. Because females are in
many societies less valued than males, a plethora of health problems
arise. One of the most blatant examples is the abuse of amniocentesis
in India. A recent Indian report states that 7,999 of 8,000 fetuses
aborted after amniocentesis were female. Another example is the forced
sterilization of mentally disabled women in West Germany. Such practices as these shatter the common myth of the neutrality of science and
technology.
Pressure to conform to certain standards of beauty-beauty being
one of the chief societal measures of a woman's worth-can incite
women to do great harm to their health. Black women in Senegal, living
under the colonial legacy that light-skinned women are the most desirable, use dangerous compounds to depigment their skin. Fat women are
urged to become thin by surgical and other means that can damage
them permanently. Women working to counter this destructive situation
urge that it is society that needs changing, not women's bodies.
Women's health is often endangered by something more fundamental than the demands of beauty. Work-both the quantity and the conditions under which it is done-can wreak havoc on a woman's well-being.
For example, in India, women do most of the cooking. A lot of cooking in
rural areas is done over a wood or dung fire, often in unventilated structures. The woman cook continually breathes smoke, which contains large
quantities of pollutants. Respiratory diseases are a leading cause of
death among girls and women over the age of five in India; smoke inhalation is thought to be a major factor.
In rural Kenya, women must walk many miles each day to collect
water. During the dry season, collecting water can be so time consuming
that the woman has little time or energy left for her other duties.
Refugee women, who are already under tremendous strain from
being uprooted, often face special health problems as pregnancy and
breast-feeding exacerbate their malnourished state. Also, because
refugee women are often responsible for collecting fuel and water and
for taking care of the children, they are the last to receive health carethey don't have the time to go to a health clinic.
Women's health collectives and self-help projects are helping
women gain control over their own health and bodies. They emphasize
preventive medicine, provide alternative treatments such as acupuncture
and homeopathy, make health care affordable and available, and provide
information on contraception and abortion. These groups are committed
to creating an accessible network of health resources for women.
Valuing ourselves and our health is an important part of change and
of healing. But women also need to regain the power to make decisions
regarding individual and collective women's health issues. In societies
"where looks and sexuality are used to control women, we need to
question all physical and behavioral norms imposed on us.'' Marching
against restrictions on reproductive rights, denouncing societal standards
of beauty and health, disseminating improved wood burning stoves in
India-all are examples of efforts to put women's health and control over
our bodies back into the hands of women. D
Connexions 25 Winter 1987
1
Eliminate Inequality,
(By Vibhuti Patel, Women's Centre, Bombay, India.)
Amniocentesis is a scientific technique that was intended to be used in
detecting genetic abnormalities of a foetus.
In India, it is currently being widely used
as a means for sex-determination. By comparison to other countries, amniocentesis is
quite inexpensive in India. Hence, not only
upper class women , but even working class
women have access to the test. A recent
survey of the slums in Bombay revealed
that when women found out their foetus
was female, many chose to abort. Many
argued that it was better to spend a bit of
money now for an abortion than to have to
pay a fortune for a girl's future marriage.
The controversy began a few years
ago when the results of several investigative reports were published in popular
Indian magazines and journals. Many of
the results were horrifying. Of 8,000 abortions following amniocentesis, 7,999 were
found to involve female foetuses. In addition, between the years 1978 and 1983, it
is estimated that 78,000 female foetuses
were aborted after sex-determination tests
in India.
The government and private practitioners involved in this lucrative trade justify the sex-determination test as a measure
for population control. Women have
always been the ones burdened with the
effects of family planning policies. Harmful
effects of pregnancy tests, contraceptive
pills, anti'-pregnancy injections, and unhygienic camps for mass sterilisation of
women are just a few of the drawbacks
often overlooked by enthusiasts of family
planning policy.
India has a history of killing female
children (dudhapiti) by putting opium on
the mother's nipple, by putting the afterbirth over the child's face , and by illtreating its daughters. Even today, female
members of the family get inferior treatment as far as food , medication, and education is concerned. When a girl grows up,
she is further harassed about her dowry.
Many social scientists ask whether or not it
is better to die rather than be ill-treated.
In the words of Dharam Kumar, "Does the
birth of...millions of unwanted girls
improve the status of women?" To think
that it is better to kill a female child or
foetus than to have a child whose sex is not
highly valued in society is fatalistic. Next,
2
Connexions 25 Winter 1987
people will rationalize that it is better to
kill the poor rather than let them suffer
poverty and deprivation! How horrifying!
But what can be the long-term implications if such trends continue? Won't it
further aggravate the already disturbed
sex-ratio? There was a large and steady
decline in the female/male ratio in India
between 1901 and 1971. Between 1971 and
1981, there was a marginal increase in the
ratio, although women are still outnum- •
bered by men. [India is one of the few
countries in the world where the femaleto-male ratio is declining.) Economists
often say that if the supply of women is
reduced, women's status will be enhanced.
According to this logic, women won't be
burnt alive because of insufficient dowrybecause they won't be an easily replaceable
commodity. But the economists forget the
socio-cultural milieu in which women have
to live. A society that treats women as
mere sex objects will not treat women in a
more humane way just because they are in
scarce supply. On the contrary, in many
local communities, there is a negative
correlation between the female/male sex
ratio and the incidence of rape, abduction,
India
Not Women
"Don't kill your daughter after sex-determination tests."
"Stop sex-determination tests offetus in the womb. "
and forced polyandry.
Another argument in favor of sexdetermination tests is one which touts the
myth of the ideal "balanced family." It is
argued that women who have one or more
daughters should be allowed to abort their
daughters and try again to produce a son.
This concept of "balanced family" is
extremely sexist and very frightening.
Would a couple with one or more sons
undergo amniocentesis to get rid of a male
foetus, just so that they could have a
daughter in order to balance their family?
No, never!
Time and again it is stated that
women themselves enthusiastically go for
the test out of their own free will. "It is a
question of a woman's choice." But, are
these choices made in a social vacuum?
Indian women are socially conditioned to
believe that unless they produce one or
more male children, they have no social
worth. They are harassed, taunted, and
even deserted by their husbands and inlaws if they fail to produce a male child.
Thus, their 'choices' are limited by their
fear of ridicule by society. It is true that
feminists all over the world have
demanded the right of women to control
their own bodies and choose whether or
not to have children. They have also fought
for free, legal and safe abortions. But these
issues should be viewed in a different context in Third World societies because
imperialism and racism are often major
forces working to control coloured populations. Population control advocates often
endorse women's rights and then divert
attention from the real causes of the population problem: the lack of food, economic
security, clean drinking water and safe clinical facilities. These factors have created a
situation where women must have between
two and six children in order to have at
least one surviving male child. This is the
root of the population problem.
Abuse of amniocentesis shatters the
myth of the neutrality of science and technology. Just as the invention of atomic
energy was used to destroy Hiroshima and
Nagasaki, so could sex-determination tests
be used for female extermination.
We at the Women's Centre are
undertaking educational campaigns to help
combat this problem. Most women's
groups feel that amniocentesis should be
permitted only under strict governmental
control and only for the detection of
genetic abnormalities. To consistently campaign against the notorious activities of
money-minded doctors and the antipathy
of the government, the Forum Against
Sex-Determination and Sex Preselection
was formed in Bombay in 1986. As a
result, the issue has gained nationwide publicity and the government has begun to
respond favourably. In March 1987, a committee was appointed to study the proposal
to stop the misuse of sex-determination
tests. We are hopeful that the government
will help to prevent the situation from
leading to further female extermination. D
Contact:
• Women's Centre, 104B Sunrise Apt.,
Above Canary Bank, Nehru Road, Vakola,
Santacruz (East}, Bombay 400 055, India.
Further Reading:
• "Action Against Sex-Determination and
Sex Preselection," Womennews, newsletter
of the women's centre, Bombay, India,
August 1987.
Connexions 25 Winter 1987
3
Britain
Robbed of Colour
(From "Robbed of Colour," by Sarojini
Ariyanayagam in Spare Rib, British feminist monthly, #173 December 1986.)
As a Black person, the last thing I
would want is to turn white. Yet this is
precisely what is happening to me. I am a
33-year-old Tamil woman from Sri Lanka.
I am very dark-skinned. At the age of 17, I
developed vitiligo, a condition in which
cells in the skin stop producing pigment.
An estimated 50 million people throughout
the world have this condition, yet most
people have never heard of it. This is probably related to the fact that, although
vitiligo can strike anyone regardless of
colour, it is Black people in particular who
bear the brunt of its traumatic psychological effects. For sixteen years, I have been
waging a battle against a process which is
gradually robbing me of my colour and my
identity.
When the first white patch appeared
above my eye, I assumed it could be
treated by a doctor. But the dermatologist
diagnosed it as vitiligo, informed me there
was no cure, and then dismissed it as a
condition I'd "have to learn to live with." I
was heart-broken. Every new spot that
appeared on my neck, face and arms just
increased my anxiety. By 1985, I had lost
80 percent of my pigment. Can you imagine the trauma of this happening to you?
Imagine how a white person would feel if
she suffered from a hormonal condition
and her skin gradually turned black?
Perhaps at this point, I should tell
you about the nature of vitiligo. It can
affect anyone, at any age. It may be triggered off by emotional stress or physical
injury. According to one theory, the body
develops antibodies to melanin, the pigment in skin. Common sites of vitiligo are
the face, genital areas, hands and hair. It is
not infectious and often appears symmetrically. It is generally a progressive condition, although in some cases patches
remain the same for years or spontaneously
re-pigment. Vitiligo affects 1-2% of any
population. Dark-skinned people in the
Third World suffer the most from the
consequences of this condition since the
loss of pigment makes one more susceptible to skin cancer. On the whole, however,
still little is known about vitiligo. A parallel can be drawn between vitiligo and sickle
4
Connexions 25 Winter 1987
cell anaemia: as they both particularly
affect Black people, the resources for
research into those conditions is not
readily available.
As with other skin conditions, like
eczema and psoriasis, one of the main conventional treatments for vitiligo is steroid
ointments. However, these should only be
used for short periods of time as they thin
the skin. The alternative is psoralen tablets
combined with ultraviolet light (PUVA).
This drug makes you very sensitive to the
ultraviolet light for a number of hours and
can have unpleasant side-effects. Furthermore, prolonged exposure to UV light can
cause skin cancer. PUVA is also used for
psoriasis. Both these treatments have a
very limited success rate and in some cases
can aggravate the condition. In Africa and
Asia, herbal treatments are commonly used
with some success.
In my case, my mother couldn't handle what was happening to my skin; she
confused vitiligo with leprosy; so I had to
cope with an incurable and rapidly
disfiguring condition on my own. At that
point, I went into a depression that lasted
until my late twenties. I would always wear
long-sleeved clothes, and try to cover up
my neck. When I saw myself in photographs, I realised that I was "deforming"
my shoulder in order to hide my neck. I
felt myself changing into a shy, overly sensitive and defensive person. Looking back,
I wish someone had encouraged me to get
the emotional support and help I needed.
Having tried all the standard treatments various doctors had to offer, I
started the rounds of "alternative therapies." I spent a lot of money paying for
treatments. After eighteen months, I realised that I wasn't getting anywhere.
Recently, however, I've gained some hope.
I just returned from Cuba where I was
treated by Dr. Cao-he believes that
vitiligo is a psychosomatic disorder; however, the physiological consequences are
not fully understood. His treatment is
based on an extract from the placenta
called melagenina. The lotion is rubbed
into the skin twice a day, and applied
under infra-red lights once a day for 15
minutes. The protein helps speed up the
oxidation process in the chemical pathway
of melanin production, thus stimulating
melanin synthesis and multiplication of
melanocytes.
After three months of treatment, my
condition improved remarkably. It is hard
to believe that only a year ago I had almost
given up hope. The effort involved in
"making up" for the outside world and trying to look "normal," had exhausted me. It
was a lonely struggle, and I was too
ashamed to talk about it. I helped to organize the Vitiligo Group because I needed to
talk with people whose condition was similar to my own. For most of us in the group,
it was the first time we'd met anyone else
with vitiligo. We found we were all saying
the same things and facing similar frustrations. The silence and pretence was over.
Being together, we could take some positive action, and begin research into all
aspects of the condition. Meeting in this
group has changed our lives.
We are now a national charity of 400
members, including a medical and research
team. At least 75% of our members are
women even though vitiligo affects both
sexes equally. The conditioning we've
received as women about the importance
of our appearance makes us react to
vitiligo differently than men. Everywhere
Ingrid Pollard/Spare Rib
we look, we are presented with images of
the model woman, no blemishes, perfect
skin, beautiful looks, and almost habitually
we adapt to the social norm. Women in the
group take "naturally" to camouflaging
their "disfigurement," dying their hair.
Women with vitiligo often feel very
desperate about sexual rejection. A couple
of women even tried having their white
patches painfully tattooed.
While I was in Havana for three
months, I met many other vitiligo sufferers
from Venezuela, Mexico and Brazil. Some
had already started re-pigmenting which
was very encouraging to me. Dr. Cao
advised me to give up camouflage make-up
in order to keep my skin clean for treatment. I hadn't done that for 15 years! It
was wonderful to be accepted as I am.
Unlike in this country, people in Cuba
didn't stare at me because of my
disfigurement. In that society, you're not a
freak for looking different.
You 're
accepted for who you are. I was very lucky
to receive the treatment free as a reward
for my work with the Vitiligo Group.
I have a tremendous amount of hope
and believe that there is a potential in
melagenina for curing vitiligo. With further
research and expertise, its effectiveness
could be increased and it could be made to
work faster. A dermatologist from England
has decided to visit Dr. Cao in Cuba to
study the progress of his patients and his
methods of research. Hopefully, it won't be
long before British vitiligo sufferers will
have access to the sort of treatment available in Cuba. □
Further Reading:
• Vitiligo and Other Hypomelanoses of the
Hair and Skin, By Jean-Paul Ortonne, Plenum Medical Book Co., New York, 1983.
Connexions 25 Winter 1987
5
Change the Mentality,
Not the Skin Color
(Translated from Fippu, Senegalese feminist trimestrial, no. I July 1987.)
In the 1970s, skin-lightening in Senegal was the cause of much debate, and a
source of embarrassment for many. However, now that "Black is Beautiful" has
long since ceased to be a rallying cry for
the world's blacks, skin-lightening is once
again in fashion. Beauty and medical
experts alike tell of the wonders of skin
lightening, promising a better love life and
improved self-esteem. This advice is given
much to the dismay of those in the
women's and social service communities,
who are concerned that these experts never
mention the dark scars and blemishes that
mar the skin after these often toxic products are applied. They speak only of the
glamor of having clear, even-toned skin,
not of the mercury poisoning, lupus and
blood disease. These are only some of the
many ailments that often afflict those who
choose to chemically lighten the color of
their skin.
Skin is composed of two layers: the
dermis and the epidermis. The epidermis,
which contains an immense network of
nerve endings, is the outer layer which protects the sensitive dermis underneath from
extremes of temperature and from the
sun's harmful rays. With only basic care,
the skin can retain its protective and elastic
qualities for years.
The products used for skin lightening, however, break down the skin's natural
protective barriers. Skin lighteners contain
mercury salts, peroxides, and other
ingredients which are unspecified. Some
methods involve cortisone injections or
topical applications. All of the compounds
are dangerous, particularly those whose
chemical compounds are not completely
known. Treatment of the disorders resulting from the use of these compounds must
be given under strict medical guidelines,
which is often painful and costly. This is
because the products used for treatment in
Senegal are either in pommade form
(cream), or in solid or liquid soaps, where
the methods of application and use can
vary greatly from one woman to the next.
Skin lightening is usually done in
three steps. First, the product (or products) must be applied and allowed to
remain on the skin all ·night long to facilitate the depigmentation process. The epidermis must be modified in order for
depigmentation to begin. Next, on the following day, an even stronger combination
of products is applied. The length of time
6
Connexions 25 Winter 1987
the products remain on the skin depends
upon the desired effect . The final step
involves the maintenance of the depigmentation process. Creams are not usually
used at this stage, since maintenance is
achieved by the use of various soaps and
skin cleansing products.
Accidents which result from the use
of these products abound, in spite of the
fact that beauty experts insist that skinlightening is just another "beauty treatment." In Dakar, Senegal's capital, these
accidents account for I% to 2% of all dermatological consultations. They include
toxic reactions to the products, damage to
blood vessels and the entire circulatory system, with injuries to one or more major
organs such as the heart, liver or kidneys,
and to diseases of the veins from the prolonged use of mercury salts, which can
bring about many types of neurological
disorders. Not to mention what can happen during treatment of these maladies:
there is always the risk of serious postoperative infection.
Senegal
"... women with clear, light skin have more
sex-appeal than others: we notice them
more! In fact, I began the skin-lightening
process because I know some women who,
having naturally dark skin, weren't beautiful, but who became very seductive from
using the products."
Many Senegalese women like Khady
feel pressured to lighten their skin so they
will be more attractive to their mates. A
large percentage of women who use the
products, in fact, are women whose husbands have brought the skin-lightening
techniques home for them to use. Women
in Senegal are still valued more for their
ability to attract men and bear children
than for their other qualities.
Men such as Lamine, age 40, make
dark-skinned women feel inferior and unattractive. Lamine, an intellectual, has a
dark-skinned wife, but he doesn't miss any
opportunity to tell either his wife or his
friends that he has a firm intention of marrying a second time, and this time, a lightskinned one!
"J prefer light-skinned women, and that's
that!" he says.
While some may prefer light skin
and extol the virtues of skin-lightening products, the women's community will continue to speak out against the practice.
They say it is threatening to the Black race
itself and an embarrassment to the country
whose former president, Leopold Senghor,
was one of the founders of the Negritude
[Blackness] movement. Skin lightening, as
Marietou, age 45 , says:
Yet skin-lightening continues to be
widely practiced in Senegal. Why? Some
apparently feel that beauty is worth achieving at any cost, and to them, ebony-colored
skin is not beautiful. Even though some
men are now using the skin-lightening products, the majority of the users are women,
from all age groups and social backgrounds.
Khady, a 22-year-old Senegalese
woman, tells us why she took the risk and
lightened her skin:
" ... is sad for a country that has always been
on the cutting edge of the war for the revitilization of the black race... and the degree of
skin lightening coincides with the degree of
alienation: the more light-skinned you are,
the more you are considered as an object to
covet! We must enlighten the women as well
as the men and reverse the canons of
beauty... Me, I am black and fit quite well in
my skin ... "
Marietou's advice to the women of
Senegal? "Changer de mentalite et non pas
de teint" (Change the mentality, not the
skin color). □
Contact:
• Fippu, a Senegalese feminist trimestrial,
B.P. 4163, Dakar, Senegal.
Fat Women Fight Back
Britain
(From SpareRib, British feminist monthly,
No. 182, September 1987.)
We are fat women who want to challenge the myths about fat. We want to
stress that fat is not always a question of
personal choice and control; neither is it a
visible sign of failure. The issue for us is
not why we are fat, but why we are treated
badly because of being fat.
Contemporary Western culture promotes an increasingly thin ideal; we have
found no positive images of fat women in
the mainstream media. Quite the contrary,
women's magazines and the media in general just focus on how to get rid of fat. In
a society where looks and sexuality are
used to control women, we need to question all physical norms imposed on us. We
should work towards self-acceptance and
self-love irrespective of the size of our
bodies.
A thin woman may suffer because
she cannot attain an impossibly thin ideal.
Fat women, however, are harassed and
discriminated against regardless of how
they themselves feel about their bodies:
society at large thinks that there is something fundamentally wrong with fat
women.
In Britain, fat women are continually
pressured to lose weight. Moreover, fat
women experience direct and indirect
discrimination in job selection and harassment at work. Fear of ridicule often
prevents us from taking part in sports and
leisure activities such as dancing and swimming. Public transport and the design of
public spaces often excludes fat people;
seats are too small and there is very little
space in pubs, restaurants, cinemas. In
school, fat children can be ridiculed by
peers and stereotyped by teachers. The
majority of clothes shops sell nothing we
can wear. The media degrade us, defining
us as a problem which needs to be eradicated; we are stereotyped as lazy, pathetic,
out of control, stupid, ugly, jolly, maternal,
asexual or sexually ravenous.
On top of all this, fat women are
often thought of as being greedy. Because
body size is often mistakenly linked with
food consumption, fat is defined as an eating disorder. While some fat people, like
some thin people, are or have been compulsive eaters, many do not have problems
with food. In fact, most fat people know
that we do not necessarily eat more than
most thin people. Yet both the diet and
medical industries promote the idea that
no matter how little a fat person eats, it is
too much if she remains fat. We have to
examine whose interests are really being
served by this idea. The market is flooded
with diet fads, pills and foods. The diet
industry is multinational and extremely
profitable. Ironically, the highly profitable
Weightwatchers is owned by a food company. Furthermore, an increasing number
of researchers from the Medical Research
Council and the Department of Health
Investigating Committee have come to the
conclusion that diet foods can be not only
expensive and ineffective, but outright
dangerous.
Good health is usually cited as the
most important reason for losing weight.
Fat women are perceived as medical prob-
!ems; regardless of whether we have a
sprained thumb or a common cold, our ailments are automatically attributed to our
fat. We are often denied proper treatment
until we lose weight; then we are mutilated
in the interests of "good health." We know
that some fat women have had their jaws
wired, many more · have used and become
addicted to diet pills, and some have even
undergone plastic surgery. Such procedures
often turn healthy fat people into ill thin
people. Side-effects include malnutrition,
diarrhea, vomiting, hernias, stomach perforation and spleen injury. It is an indication of the suffering and humiliation fat
people experience in their lives that many
are prepared to undergo these operations.
So it is not necessarily fat, but fat
oppression that can damage our health. We
are physically and emotionally hurt by
external and internalised oppression, and
then we are blamed if this results in ill
health-as if health or size were simply a
question of individual choice and control
and were divorced from social and political
issues.
If you have dieted a lot and always
end up getting fatter, you learn that you
don't have a choice about your size: either
you can blame and hate yourself or you
can choose to challenge those that oppress
you and refuse to be victimised. It is a political act for a fat woman to get angry
about the way she is oppressed and to stop
believing she deserves such pain and degradation.
Most of us might already be challenging fat oppression in our lives, but it is
important that we organise collectively to
ensure that our views are made part of a
wider political agenda. We can attempt to
build a network of support groups and
activities. We can set up local swimming
and exercise classes for those fat women
who choose and are able to participate in
such activities. We can challenge the
clothes industry, which fails to meet our
needs (even though about half the women
in this country take a size 16 or over) and
encourage the setting up of co-ops that
make clothes fat women want to wear. We
need to challenge the medical profession
and demand our right to adequate health
care. We can campaign against oppressive
industries which exploit, abuse and humiliate fat women. We can challenge negative
representation of us in both the mainstream and alternative media.
We must make ourselves and other
people aware of the fact that being fat and
beautiful are not mutually exclusive; people
should love us for who we are and not in
spite of the fact that we are fat. To stop
punishing ourselves is just a beginning-we
still have to affirm our right to, quite
literally, take up space. We demand pleasure and fulfillment as fat women now, not
in some thin future. It is society that has to
change, not us. □
Further Reading:
• "How Society's Obsession With Thinness is Consuming Women," Herizons,
Canadian
feminist
magazine,
October/November 1986.
Connexions 25 Winter 1987
7
Screaming in the Wind
(From Makara, Canadian
three/Number one.)
women's
quarterly,
Volume
The following are excerpts from taped conversations between
Molly Dexell and MAKARA's Nora D. Randall. Molly spent
almost twenty years going in and out of mental institutions.
Q: Why do people go into mental institutions?
A: There are two reasons why people go into a mental hospital.
Either they can't function, or they do something that looks crazy
to other people. Now suppose you've got a mother of six kids
who is so depressed that she can't get up in the morning.
There's a two-year-old starving, and the mother still can't get up.
Oftentimes the mother will be institutionalized because she can't
cope with everyday life. Why couldn't the family just hire someone to help out with the kids and give the mother a chance to get
better? She could visit her shrink at the day hospital and come
home at night. It is very hard to deal with getting well and raising children simultaneously. It was hard enough for me and I
only had one child. They'd be saving money by not institutionalizing her, and they could keep the whole family together.
Q: How do you see the relationship between psychiatrists and
mental patients?
A: People who haven't been mentally ill are not totally aware of
what the whole thing is about, although some act as though they
do. Psychiatrists don't have a chance of being successful at helping mental patients until they accept the fact that only the mentally ill really know what their sickness is all about. Once they
have had one year of college psychology, many student doctors
diagnose themselves as being "schizophrenic", "catatonic", and
all that shit. I've had some of them say to me, "I'm a potential
mental patient." Well, sure, the whole world is. I say,"Do you
know what it's all about to hear a voice? Do you know what my
voice is all about?" It irks me so badly, to hear that kind of
drivel. Another thing I've learned from experience is that you
don't tell psychiatrists in the hospital about anything important.
You don't even tell them you don't like baked potatoes. You talk
about all kinds of things you think they want to hear. You have
to go to them for your medication, you see, you're tied to them;
you need the medication and you know it, and there's no way
you can get it without going to a shrink.
The job of getting well has been taken right out of your
hands-the psychiatrists handle it. It's really your problem and
you're the one who knows it. There isn't a psychiatrist who
knows more about me than I do. The only thing that's going to
save mental patients is mental patients. The psychiatrists are
there to help save themselves. But they take it out of our hands
and blow us out with shock treatments and pills and all the rest
of it. That is no way to cure mental illness. That's proven by the
return to institutions of so many mental patients-old mental
patients who have had the problem recur because it isn't properly fixed the first time: You can have a breakdown and another
breakdown and another breakdown, and eventually you yourself
must work your way out of it.
8
Connexions 25 Winter 1987
Q: Don't you think mental patients could work their problems out
sooner if the way they were treated in the hospital wasn't so
literally sickening?
A: Yeah, it's really a lousy setup. I had hope because I had a
good psychiatrist. If you've got a good psychiatrist, someone who
values intelligence, she or he is concerned about fear. Fear is the
greatest emotion that mental patients have. Anger is another
great emotion. And the anger is a result of your fear. The fear is
beyond belief... beyond the conception of the ordinary person.
Q: Do you think it is fear of the actual illness itself, or fear of how
you'll be treated because you are sick?
A: Well, both. The intense illness is frightening. But I think it's
intensified in the hospital.
Canada
Q: Knowing what you know now, if a doctor ordered shock treatments for you, would you kick up a fuss?
A: No way. If you kick up a fuss in a mental hospital, you get
locked up. I wouldn't kick up a fuss in the hospital. That's the
craziest thing I've ever heard. Why, they'd just pick you up and
carry you in, that's all. I've seen a 70-year-old woman, screaming and fighting, picked up and carried in. Once you see that
happen, people get educated. That's the biggest shock in a mental
hospital. I hesitate to compare these-it sounds a little
paranoid-but it must be the same feeling that political prisoners
had during Nazi Germany, during the extermination. People
were picked up and terrible things happened to them, while the
rest of the world was ten miles away and didn't know what was
happening.
It's the same at Riverview. Totally helpless, cut off, nobody
relating to you, nobody understanding what's happened to you,
and there's this screaming in the wind. That's a feeling you have,
and you don't ever get over it. It never leaves you. I would be
very, very slow about putting anyone in a mental hospital for the
first time. When you go, you .see things and learn things you
never forget. No matter what you do, where you go, you're
always afraid you'll be put back. Your whole life is taken totally
out of your hands and it's put in the hands of ruthless people.
When psychiatrists learn to relate to their patients, then they will
have learned a little about psychiatry.
Beyond Sound
My day is a snare
In which I am caught
Struggling.
At dawn I am revived
To continue
What has become to me
A life outside of life
Where my soul screeches
To unimagined heights
And instinct holds me back,
Puts on the brakes,
Till gathering strength
I quietly descend to the glassy surface
And I remain,
Healing myself
By the steady routine of my existence
And yet,
I am not healed,
For a word
A distant threatening sound
Q: Is there a place for mental hospitals?
A: Not called mental hospitals. There should be a place. Someplace restful, where they could have a holiday-Hawaii. D
Shoots me off again
Shattering the cobwebs
That enfold me
Encircle me
Bind me
To some hidden sorrow
That lies there in a stupor
At the back of my head.
There is no word
That accurately describes
The feeling of foreboding that I once had
That now slides past like some reptile
Nudging at the corners of my eyes.
Let me look away;
Let me see the things I love.
How wonderful!
How beautiful!
But it is still there!
When will I feel safe again?
Never?
(By Molly Dexell)
All graphics by Marie Falksten
©
Further Reading:
• Women and Therapy, a feminist quarterly, Hawthorne Press, New York.
• I'm Not Mad, I'm Angry, Dorothy Smith
and Sara Davids (eds.), Press Gang,
Vancouver, B.C., 1975.
Connexions 25 Winter 1987
9
Sterile Without Consent
(Excerpted from Connexions' interview with Theresia Degener,
December I 987.)
Theresia Degener is an active member of the West German
disabled movement. She is particularly interested in the issues surrounding the involuntary sterilization of disabled girls and women.
She has published a book about disabled women and has written
an article on this subject which was published in Emma, a West
German feminist magazine, in August 1985. Theresia is currently
a law student at the University of California, Berkeley.
In 1984, the West German media started to pay attention
to the issue of sterilization. This was partly due to the discovery
by htstorians that many of the girls in schools for the mentally
disabled had been sterilized without their consent or against their
will. After these findings were publicized, a television program
"Panorama" was devoted to this topic. On "Panorama," a
mother explained that she had had her disabled daughter sterilized at the request of her daughter's teacher. The teacher
requested sterilization because the children were going on an
overnight field trip and he did not want to be responsible in the
event that the girl engaged in sexual activity and became pregnant.
In fact, many institutions in West Germany require the
sterilization of mentally handicapped girls as a prerequisite for
admittance. The institutions don't want to deal with the possibility of a pregnant disabled woman. Parents of disabled teenagers
are often intimidated by the sexuality of their children and are
fearful of a potential pregnancy.
"Panorama" alerted the public to these issues-many
Social Democrats and much of the alternative press were
horrified at these findings. Many who protest this abuse of sterilization draw parallels between the current situation and the
forced sterilization that occurred under the Nazis. An estimated
400,000 people were sterilized against their will or without their
consent during the Nazi era. Currently, there is a heated debate
about whether or not the federal government should provide
compensation for those who underwent forced sterilization.
The present West German criminal code clearly states that
sterilization is illegal unless it is performed with the consent of
the affected and if this consent is not against ethical principles.
Sterilization against a person's will or without her consent is only
permissible if there is a present danger to the health of that person. However, some people claim that there is a gap in the law,
in that it does not say anything about those who are mentally
unable themselves to give consent. Some intermediate courts
have ruled that the consent of the disabled can be replaced by
the consent of the parent or _legal
representative in cases
where the disabled person is incapable of making her own decision. This is not legal, however, as the law does not allow for this
option. The legal system in West Germany is not a case system
like the United States where the rule of precedence must be followed. Courts in West Germany do not look to precedents set by
other courts, but rather they must find the answer in the law
itself.
Lebenshilfe, the largest organization for the parents of the
disabled, is one of the main proponents of involuntary sterilization. It was founded in the 1950s and it runs "sheltered
10
Connexions 25 Winter 1987
workshops"-a place where disabled people are employed. It
runs several other institutions and even has its own publishing
house. Lebenshilfe and many other parents not organized in
Lebenshilfe want a new law legalizing the sterilization of the
mentally disabled because they don't want their children to
become pregnant. Many of the parents feel that because they
have already exerted so much energy raising a disabled child,
they don't want the burden of raising their children's children.
They claim that sterilization is in the best interest of the kids
and that there is no place within the institutions that could
accommodate a pregnant mentally disabled woman. The common morality on this subject is that the mentally disabled db not
have a right to reproduction.
In the 1960s and 1970s, not much was known about how
many people were affected by this practice of sterilization, but
recently teachers in Hamburg have revealed that about 30% of
the girls in special schools for mentally disabled children have
been sterilized. These girls are less than 18 years old-most of
them are less than 14. It has been easy for parents to have their
kids sterilized; doctors agree readily. On the other hand, for
able-bodied women, it is very difficult to get a sterilization. If
they are under 18, it is illegal.
The federal government started an investigation to find out
how the federal states and institutions are dealing with the problem. A special board was created to work out a statute which
allows for sterilization without consent. Special education experts
say also that what has been done in the past should be made
legal.
One major concern parents and institutions have is rape.
Many mentally disabled women are raped in institutions, by relatives, and in the streets. However, there are no available statistics
on the subject. Mentally disabled women are in particular
danger because they cannot communicate the same way we communicate; they can be easy victims. Proponents of sterilization
claim that they want to prevent the repercussions of rape,
namely conception, since many of them are Catholic and cannot
agree with abortion. I think it is very cynical to deal with the
problem of rape by sterilizing disabled women.
Eugenics is another concern. There is a big discussion
about eugenic thinking and of new developments in the fields of
genetic engineering and reproductive technology. Udo Sierck,
who is disabled and has done a lot of work on this issue, has
discovered that some genetic counseling offices which are provided by the state in West Germany also provide sterilization
recommendations for other doctors. The recommendations are
most often based on social behavior: If you are in a special institution, if your father is an alcoholic, if your uncle is unemployed,
if your brother is also in a special institution, you are diagnosed
with an inherited disability, and sterilization is recommended.
The eugenic arguments used by these counseling offices are
currently a hot topic in West Germany, because they remind
people of the population control the Nazis planned. Some papers
were stolen from some of these offices and published, which was
very embarrassing for the people working there. They had
difficulties saving their jobs and justifying genetic counseling.
There are a few people, such as progressive educators and
church organization members, who criticize the current
approach. They propose that we look to other countries for
West Germany
examples of possible alternatives. In Denmark, for instance,
there is something called "protected marriages"-houses are provided for mentally disabled couples so that they can live
together. Special attendants take care of their needs and the
needs of their children. The government provides these
services-Denmark is much more of a welfare state than West
Germany. Similar programs are planned in the Netherlands and
at least two similar programs exist in West Germany. Reports
indicate that these programs are highly successful. The main
drawback to the development of further programs is the lack of
available funding. This is a big issue in West Germany right now
as the social welfare law does not explicitly allow for funds to be
spent in this way. In addition, most of the disabled parents need
supplemental assistance as they earn minimal wages.
Until recently, disabled people in West Germany were
discouraged from having sexual relationships. Many books have
been published that state that the disabled should not have the
right to sexuality. In many institutions, methods were used to
distract disabled people from their sexual feelings. Although it is
currently said that the mentally disabled have a right to their sexuality, people are now trying to regulate the circumstances under
which the disabled are allowed to have sexual relationships.
There are some people who are supportive of the right of the disabled to sexuality. Several organizations offer services to disabled people who request reproductive counseling. They provide
advice on sexual problems and planned parenthood, and help
parents to educate their children about birth control.
The conservative West German government is trying to
pass a new custody law. There is a provision in that law that
states that for disabled people who are unable to give consent for
sterilization, the parents or legal representative have the power to
approve the procedure. The government wanted to enact this
law in September 1987, but was unsuccessful due to the resistance of the Green and Social Democratic parties. These parties
are very sensitive to this issue in part because of their work to
get compensation for Nazi sterilization victims. The Greens and
Social Democrats are supportive of the reforms in the new custody law except the provision dealing with the sterilization of
disabled people. The government had therefore excluded the
controversial provision in order to pass the reform of the custody
law. But the government will continue its fight to legalize the
involuntary sterilization of the disabled.
I think that one major problem is that many people believe
that the reproductive choices of disabled people are a public
issue and not a private right. There is also a prevailing attitude
that disability is abnormal and therefore unacceptable. If one
examines current developments in the fields of genetic engineering and reproductive technology, one can see that people have
(cont. on p. 28)
Connexions 25 Winter 1987
11
Restricted ''Choice''
Ireland
(Submitted by Pauline Ryder: The Dublin
Well Woman Centre, Dublin, Ireland,
October 1987.)
The Dublin Well Woman Centre was
founded in 1978 with the aim of providing
medical care, counselling, fitness programs,
and other services related to women's physical and mental well-being. Our philosophy is based on the principle that women
have the right to take control of their own
physical and mental health. In 1978, access
to family planning information was
severely restricted in Ireland. The Well
Woman Centre sought to help bridge the
gap between the limited services available
and the demand from Irish women for
easily accessible birth control. To date,
78,000 women from all over the country
have used our services. In addition, we
provide educational leaflets on aspects of
health including contraception.
Up until January, 1987, we provided
non-directive pregnancy counselling to
women coping with unplanned or
unwanted pregnancies. Our aim was to
create a safe, private, and accepting atmosphere in which a woman could discuss all
her options (including the option of abortion, which is illegal in Ireland). In cases
where a woman decided to have an abortion, we referred her to approved, legal
clinics in the United Kingdom. We also
acted as a telephone service for people
wanting information on abortion.
In October of 1986, a High Court
Action was taken against the Dublin Well
Woman Centre and Open Line (the only
other agency in the Republic of Ireland
offering this type of pregnancy counselling)
by the Society for the Protection of the
Unborn Child (SPUC). This action was the
result of an amendment to the Constitution
in 1983 which gave the foetus a right to life
equal to that of the mother. This amendment was sought by SPUC, which succeeded in winning the support of the main
political parties. The outcome of the High
Court case has resulted in an injunction on
our Pregnancy Counselling Service and the
closure of Open Line. Indeed, we are restricted by law from giving any information
concerning abortion. Recent statistics suggest that this injunction has done nothing
to reduce the numbers of Irish women travelling to England for abortions. The
injunction has pushed access to information underground (there is a national campaign which has set up a country-wide network). It has also increased the trauma and
stress women have to go through in order
to obtain an abortion.
The long term effects this will have
on women and their physical and mental
well-being are yet to be seen. It is currently
a civil offense to give out information on
abortion; women are made to feel like
criminals. We are being denied a basic civil
right-access to information.
12 Connexions 25 Winter 1987
We have appealed the High Court
decision to the Supreme Court, and are
awaiting the hearing. The legal fees
involved are astronomically high and the
success of our appeal depends on raising
the funds required to see the case through.
Any contributions to help us in our plight
would be most welcome.
Please send to:
Dublin Well Woman
73 Lower Leeson Street
Dublin 2
Ireland
(From Women's News, Irish women's
magazine, July/ August 1987, Belfast, Ireland.)
When the Society for the Protection
of the Unborn Child (SPUC) launched its
successful campaign to amend the constitution of 26 counties to guarantee the right to
life of the unborn, Southern politicians
assured us that this was not an attack on
women's rights, but merely an action to
prevent the courts from declaring the old
1860 Act (making abortion criminal)
unconstitutional. However, as many of us
feared at the time, the amendment was
only the first step in a much longer-term
SPUC strategy to deny women access to
information on both contraception and
abortion. In 1983, SPUC attempted to
intimidate women from seeking advice on
these matters by picketing family planning
centres and women's clinics. In 1986, they
went a step further and began a legal campaign to stop women's clinics from providing any services of this nature.
SPUC initiated court proceedings
against The Well Woman Centre and Open
Line Counselling. The case was heard by
Justice Hamilton, who found in favor of
SPUC; he ruled that all other constitutional
rights are held secondary to that of the
right to life of the unborn. The judgment
therefore denies women the constitutional
guarantee and equal right to life, the
guarantee to privacy, and the guarantee of
access to information.
Thus. from December 1986, nondirective
pregnancy
counselling
has
effectively been banned from twenty-six
counties. Furthermore, if the decision is
implemented literally, it would mean a distressed pregnant woman could not get
information on abortion from her closest
friend without potentially engaging in a
"criminal conspiracy." Doctors advising
patients on these matters could be
prosecuted. Certain contraceptives such as
the IUD and the morning after pill could
be banned. Popular newspapers and magazines could be censored. The fearsome
scope of the judgment and the danger it
poses for civil liberties has provoked an
angry response from women who are determined to defend their rights. It has also
brought the realization that SPUC must be
stopped now.
The Defend the Clinics campaign
began functioning as soon as SPUC's court
action was announced. The aim of the
campaign is to make the judgment against
the clinics unpopular and to create a network of information needed to restore the
challenged service. The Dublin-based
national committee has now distributed
hundreds of information packets (giving in
pamphlet form information previously
offered by the women's clinics), thus defying the injunction.
We believe that in order to succeed
in our campaign, not only must the
women's movement of the North and the
South unite, but all working class organisations, political parties, and progressive
forces in Ireland must fight SPUC's agenda.
If SPUC is not stopped, women will suffer
yet more defeats at the hands of the right
wing, and the outlook for the future of
Irish women will be unthinkable. □
Israel
(Submitted by Awatef Barghut,
clinic nurse, Nazareth, Israel.)
health
It is impossible to separate any subject in Israel today from the political and
social reality in which the economic crisis;
continuing occupation of the West Bank,
Gaza Strip and Golan Heights; the war in
Lebanon; and the continuing oppression of
Palestinian people are major factors. With
respect to abortion, women's reproductive
rights are limited. In order to have an
abortion in Israel, a woman must appear
before a committee consisting of a doctor,
psychologist and social worker, and receive
their permission. The only grounds for
approval are if there is severe danger to
mother or child, if the pregnancy is a result
of rape or incest, if there are special religious reasons, or if the mother is mentally
incompetent. The "social clause" of the law
permitting abortions for socio-economic
reasons, by which most abortions were performed in the past, was cancelled in 1978.
I can't say that there is a policy of pressuring Arab women to abort, but people say
that despite the law, all Arab women can
get an abortion when they request one, as
opposed to Jewish women, who are pressured to have the child. Jewish women are
told they can put the child up for adoption
if they don't want to raise it. □
India
(From Manushi, Indian feminist monthly,
no. 36, 1986.)
Abortion in India was legalised in
1972. The number of legal abortions is
increasing steadily each year. Unfortunately, the number of illegal abortions
performed is also increasing. The increase
has occurred through sustained propaganda. People have been led to believe
that abortion is a trivial operation. It is
often advertised as something that is cheap
and easy to have done on your lunch
break. Abortion is projected as a procedure of little financial or physical consequence.
Commercial
interests
have
encouraged many illegal practitioners to
perform abortions.
Many people see abortion as a simple
procedure that a person with any sort of
medical
qualification-allopathic,
ayurvedic, or homeopathic-is competent
to perform. It is even said that non-medical
persons can easily learn the technique. In
spite of all the modern and safe methods of
terminating pregnancy that are available in
this country, severely damaging and often
ghastly methods continue to be used to
induce abortion. A spate of reports in the
last two years reveal that iron nails, sticks,
coconut splinters, and Fetex, a dangerous
chemical paste, have all been used by illegal abortionists. The types of injuries
inflicted by illegal abortionists are horrifying. Perforation of the uterus and injury to
the rectum , urinary bladder, intestines and
liver, severe infection of the peritoneum .
and chemical burning and sloughing of
internal organs have all been reported in
recent cases.
The havoc caused by septic abortions
continues unabated in spite of all the
powerful infection controlling drugs available now. There are no beds earmarked for
abortion cases in hospitals. Centres for
medical termination of pregnancy have to
be approved by medical authorities, but
many unapproved centres continue to function.
A report from Patna Medical College
Hospital reveals that maternal deaths due
to abortion have increased from 5.6 percent of all maternal deaths between 1961
and 1965 to 9.0 percent between 1976 and
1980. Fetex chemical paste, licensed, publicised and popularised as an abortificent
paste, has caused peritonitis, gangrene of
organs and kidney failure in many cases.
Doctors recommend that advertisements
for Fetex paste should be banned and the
product withdrawn from the market. It is
due to the inefficiency of the mechanism
for controlling drugs in our country that
after years of reporting on the fatal effects
of this paste, it continues to be licensed
and marketed. D
Hong Kong
(From Women's News Digest, June-August
1986, Hong Kong.)
The approval of two registered doctors is required for a legal abortion under
the present Hong Kong law. This law
denies women the right to make decisions
about their own bodies by allowing doctors
to impose decisions on them. Therefore,
the legal system in Hong Kong is forcing
women to cross the border into China to
seek cheap and easily accessible abortions.
In addition, the laws have contributed to
the number of women seeking illegal abortions from unlicensed doctors in Hong
Kong.
Ms. Chan, chairwoman of the Association for the Advancement of Feminism,
believes that the trend of seeking abortions
across the border is "a result of the
insufficient abortion service in Hong
Kong." Medical and Health Department
statistics show there were 28,130 legal
abortions between January 1982 and
December 1984. Among these, 70.8 percent were carried out in private hospitals,
while only 7.2 percent were carried out in
government hospitals. Just over 22 percent
were carried out in subsidised hospitals.
Ms. Chan points out that "The fact that a
high percentage of women are having to
terminate their pregnancies in private hospitals indicates the inadequacy of a cheap
abortion service." She goes on to report
that middle and upper class women have
easy access to abortions because they are
able to pay the cost, usually between
$3,000 and $5,000. Lower middle class
women are often obliged to seek cheaper,
but more dangerous illegal abortions.
"The only other viable alternative
seems to be the service available across the
border, despite the possible risks due to
lack of follow-up service." "A strong
stigma attached to pregnancy out of
wedlock shames women into getting abortions, whether they want their children or
not." It is this stigma which drives many
women, especially young women, across
the border for abortions.
Ms. Chan states that it is necessary
to challenge and change the hostility
against unwed mothers. As a more immediate task, however, she stresses the need to
provide sex education and information
about contraception to women, a task
which a responsible government cannot
ignore. D
Mauritius
(From "Medical Guide-Illness No, Health
Yes," and "Women's Minimum Program,"
Mauritius.)
"One child is enough, and it matters
little whether daughter or son, as long
as the child is healthy and strong.,,
According to the Penal code section
235, abortion in Mauritius is illegal. The
law originated in the colonial period and
should be immediately revoked in order to
decriminalize women. This is all the more
necessary because according to statistics,
every woman in Mauritius has an average
of five abortions within her lifetime.
g According to government figures, four
6 thousand women are hospitalized each year
~ as a result of clandestine abortions. Doctors estimate that approximately 40,000
women each year have an abortion, many
of whom seek cheap abortions. Unfortunately, these inexpensive abortions are
often done with utensils such as umbrellas,
knitting needles, or spokes causing many
women to suffer from complications that
can be terminal. Among the points listed in
the Women's Minimum Program, which
the Women's Liberation Movement distributed to all the major parties, was a
demand to repeal the Penal Code Section
235 immediately. □
Connexions 25 Winter 1987 13
Japan
(From Asian Women's Liberation, Japanese
feminist quarterly, No. 6 1984.)
Nineteen eighty-three was a crucial
year for women in Japan. The Ministry of
Welfare proposed legislation aimed at
tightening restrictions on abortions. The
course of events began in March, when
Representative Murakami Masakuni, who
is backed by right-wing religious groups,
announced: "Vast numbers of abortions
continue to be performed for economic reasons despite the fact that Japan has become
an economic superpower. This casts doubt
on the future prosperity of the Japanese
people. Abortion is murder. Allowing it to
continue unchecked will result in the moral
degeneration of our society. Accordingly,
abortion must be strictly controlled."
The first step toward this end was to
propose deleting the "economic reasons"
provision from the list of conditions contained in the Eugenic Protection Law
under which a woman may obtain an abortion. Proponents of the revision launched a
huge media campaign and held rallies using
such slogans as "Respect for Life" and
"Protect Fetal Life." They also methodically collected over ten million signatures
to a petition calling for the revision,
including those of legislators from all levels
of government.
The fundamental law in Japan concerning artificially induced abortions
prescribes imprisonment for women who
procure unauthorized abortions. Other provisions prescribe varying penalties for doctors, midwives, pharmacists, druggists and
others who participate in such abortions.
These provisions were first introduced to
the criminal code in 1880 as part of the
westernization Japan was undergoing at the
time. Previously, abortion had not been
treated as a legally punishable offense. In
fact, during the years 1603 to 1868, both
abortion and infanticide (which was often
sex selective) were routinely practiced by
poor rural peasants as a form of self preservation and a method of population control.
(As a result, the overall population
remained stable for almost 300 years.)
The criminal abortion laws introduced in 1880 were significant in that they
coincided with a new national policy to
westernize Japan in terms of wealth and
military strength. One aspect of this policy
called for boosting the country's population . Especially from around 1930 until
1945, women's bodies became the territory
of the state. Motherhood was a public duty;
the criminal abortion laws were strictly
enforced and even contraception was forbidden. The first priority was to ensure a
supply of labor and soldiers for the war
effort.
In 1948, the Eugenic Protection Law
was introduced. Its purpose was to control
the enhancement of desirable Japanese
racial qualities primarily through sterilization and abortion. The conditions under
which abortion can . be performed are
divided into three major categories: {I) for
eugenic reasons (existence of hereditary
physical or mental disorder); (2) for public
policy reasons (pregnancy resulting from
rape or coercion); and (3) for personal
14
Connexions 25 Winter 1987
sociological reasons (possible injury to the
woman's health from a physical or
economic viewpoint). Economic reasons
were added to these conditions as a new
category in 1949. In effect, this had led to
the realization of abortion on demand in
Japan. These demands are sometimes
based on fictitious claims of economic
hardship.
Japan's population needs changed
dramatically following World War II. Having lost its foreign territories and facing
acute food shortages, reducing the population became a national priority. Also, in
order to alleviate the increasing number of
back-street abortions and the physical
dangers these presented for women, it
became necessary to legalize abortion.
There can be no doubt that the reduction
in the size of Japanese families after the
war can be primarily attributed to abortion.
native intelligence. They worry that among
those fetuses "selfishly" aborted there may
have been geniuses who might someday
have benefited Japan's economy.
It is not enough simply to have this
offensive bill shelved. The opposition
movement is starting to prepare its own
reform proposals. Feminists have been trying to abolish the Criminal Abortion Law
and the Eugenic Protection Law altogether.
The Criminal Abortion Law is an
unjustifiable governmental intervention
into individual privacy and ignores basic
human rights. The Eugenic Protection Law
is premised on the philosophy of promoting racial purity. The net effect is to deny
women through forced abortion the opportunity to have children when they want
them, and to penalize women who choose
to terminate unwanted pregnancies. It is
important that we work for an environment which enables women to choose
One bill to revise the Eugenic Protection Law was introduced in 1972, during
the last stage of Japan's period of high
growth immediately preceding the oil
crisis. The central feature of the bill was
the deletion of "economic reasons" and its
replacement by the purely medical condition of "mental or physical health reasons." Abortion would also be allowed
where the fetus was found to be handicapped. The bill also required young
women who had never given birth to
receive advice and guidance before an
abortion could be performed. A key factor
said to be behind the bill was the shortage
of young workers to meet the demand for
labor caused by Japan's high economic
growth. From this need emerged the
national priority of increasing the country's
human resources. The bill was met with
intense opposition and was successfully
blocked in 1972 and 197 4.
In 1982, reflecting Japan's increasingly conservative political climate, the
proposal to strike "economic reasons" from
the Eugenic Protection Law once again
came to light. Conservatives say that Japan
lacks the necessary natural resources for
economic development; therefore it is crucial to utilize Japanese people's "superior"
whether or not to have children, so that
men and women together can achieve their
full potential as human beings. Contraceptives are very tightly regulated by the
government in Japan, therefore, the first
priority should be to provide better contraceptive planning and services for couples
who choose not to have children. □
Contact:
• Muvman Liberasyon Fam, Lakaz Ros, 8
celicourt Antelme Street, Forest-Side, Mauritius.
• Defend the Clinics Campaign, National
Committee, 6 Crow Street, Dublin 2, Ireland.
• The Women's Centre for Advice and
Information, 18 Donegall Street, Belfast,
Ireland.
Further Reading:
• "Irish Women Defiant Over Abortion
Rights," Out write, British women 's newspaper, Issue #55, February 1987.
• Women's News Digest, Association for
the Advancement of Feminism, Hong Kong,
June-August 1986.
The International Meeting on
Women and Health
Costa Rica
(From "The International Meeting on
Women and Health," by Maria Eugenia
Jelencic, Women in Action, an Isis International publication, 1987/2.)
About 800 women from five continents met in San Jose, Costa Rica last
May for the Fifth International Meeting on
Women and Health. The week-long meeting was organized by the Feminist Center
of Information and Action (Centro Feminista de lnformaci6n y Acci6nCEFEMINA) of Costa Rica. There was a
large representation of Costa Rican women
and Latin American women in general there were very few Asian women (about
20) and even fewer African women (no
more than l 0).
The Women and Health Movement
has developed appreciably since 1977, the
year of the First International Meeting on
Women and Health in Rome, Italy. For
· many groups and organizations, it was the
first time they had encountered women
from different countries doing work similar
to their own. The San Jose meeting was a
demonstration of the vitality of the movement. There were three central workshops:
"Reproduction Rights and Population
Problems," "Medicines and Drugs," and
"Community Health," and 130 other
workshops were proposed by the various
groups who took part in the meeting.
The initial program had to be
modified and adjusted several times in
order to allow a forum for each problem.
First there were the specific, daily problems
which confront women as a gender. In the
majority of the countries represented,
women's groups are the only place where
these problems can be confronted. The
titles of the following workshops are indicative of the issues that women's groups
take on: "Circumcision of Women in
Sudan," "Women Under Muslim Law,"
"Mental Condition and Female Condition," "Physical and Mental Illness in
Women as Resistance to Patriarchy,"
"Alternative Sexual Education," "Subjected Body/Despised Body," "Effects of
Drugs on Lactation," "Psychosocial Elements of Maltreatment of Women," "SelfHelp Groups," "Domestic Violence" and
many others. There were also workshops
on environmental pollution, the Chernobyl
and Bhopal disasters, and on abuses of the
new reproductive technologies.
It was generally agreed that the
women's
health
movement
must
significantly increase its organization and
reinforce itself as a pressure group that can
promote political change. There is a lack
of adequate instruments of communication
and of materials with content that
effectively supports health programs. The
dissemination of information to illiterate
women, especially in the rural sectors and
inner cities of the Third World must be
addressed, as lack of information is the
basis of much abuse: forced sterilization
and the use of poor women as "guinea
pigs" in experiments with contraceptives
are just some of these violations.
Isis International is working on
improving the communication of health
information to all women. In the workshop
"Audiovisual Communication as Support
for Women's Health Programs," which Isis
coordinated, several groups were cited for
making progress in this area. One of Isis's
own projects is a low-to-medium cost training workshop for health workers in groups
in the Latin American region. Ana Maria
Portugal of Peru told of a network that has
been initiated in her country to provide
audio cassettes containing programs for
women. Ilet Mujer is also promoting a
Latin American radio network, and in
India, there have been seminars in video
training for Asian activists.
The groups which participated in the
workshop on the Health Network of Latin
American and Caribbean women indicated
how valuable the creation of this network
had been in breaking the isolation of
groups working at the local level, and how
it had also helped towards coordination at
a regional level. This network started in
1984 and now includes 500 organizations
and groups in the region.
The workshop of the Global
Women's Network on Reproductive Rights,
which includes about 600 groups, was
another confirmation of the effectiveness of
the networks. "When we began to coordinate with other Asian groups we discovered
that many of the population control policies which were being implemented in
India were the same ones that exist in
other countries in the region," said one
representative from Saheli, an Indian
organization.
One great concern for women
involved in the reproductive rights movement is drug dumping. "Through the network, solidarity and vigilance among
women can be intensified," said one participant in the workshop on Drugs and
Medicines. "If we are better coordinated,
women in developed countries can exert
pressure to make sure that medicines and
contraceptives which are prohibited in
those countries are not sold in Third World
countries as they are today." In a final
document, signed by the Third World
women present at the conference, severe
criticisms were made of the majority of
health policies implemented in their countries.
One section of the document reads,
"Health policies implemented in our countries are based on profits and on power for
elites ... Added to this is the deterioration of
the economic situation of the developing
countries as a consequence of International
Monetary Fund tax policies, which are the
cause of poverty, hunger, unemployment
and lack of housing. In consequence, serious health problems for millions of people,
especially women, are created." The situation is complex. Can support for the
Women and Health Movement help to
improve the situation? Do we help to
improve the situation? We think so. In
many places the Women's Health Movement is still in its initial stages.
In the next meeting, planned for
1989 in the Philippines, it will be possible
to evaluate all the advances achieved in
these two years of work. However, in the
meantime, we must keep in contact, tighten
our bonds and work in a coordinated way.
There is no other way to achieve significant
advances. □
Contact:
• Centro Feminista de Informaci6n y
Acci6n, Apdo. 5355, San Jose, 1000 Costa
Rica.
Further Reading:
• "Conference Demands International
Health Rights," Outwrite, British women's
newspaper, Issue 60, July/August 1987.
Marie Falksten ©
Connexions 25 Winter 1987
15
Nigeria
AIDS Linked to Genital Mutilation?
(Submitted to Connexions by Hannah
Edemikpong, coordinator of the Women's
Centre in Nigeria.)
The question of where the AIDS
virus originated is a matter of intense
international debate. Some say that AIDS
may have appeared first among the green
monkeys of Central Africa or perhaps in
some backwater village in the interior of
the continent. Whatever the outcome of
the international debate, it is indisputable
that AIDS is here and is spreading ram•pantly. Seldom has a single disease put so
many people around the world at great
risk. The AIDS microbe comes in a variety
of strains and has the ability to mutate
rapidly, making the development of potential vaccines highly problematic.
16 Connexions 25 Winter 1987
Some scientists say that as many as
five million Central Africans may carry the
virus. The World Health Organization says
that the virus is now spreading to other
areas in Africa. The overwhelming majority
of Western victims still come from two
specific groups: male homosexuals and
intravenous drug users. But what is happening in Africa is quite a different story.
What are the cultural factors involved in
the transmission of AIDS in Africa? Uli
Linke, an anthropologist and researcher at
the University of California, Berkeley, says
that there is "a prevailing assumption that
the same cultural factors are at work in the
transmission of AIDS in Africa as in
Europe and the USA. .. But none of the cultural factors can explain the equal ratio of
men and women contracting the virus in
Central Africa. The bottom line in the
transmission of AIDS is the exchange of
bodily fluids, particularly blood, which
gave me the idea that it might be related to
female circumcision."
In Africa, women are noted carriers.
In a recent survey done in Uganda, of the
170 pregnant women tested, 75 percent
were found to have AIDS. Half of those
found to have AIDS had been genitally
mutilated. In Equatorial Guinea, of the 100
women who were tested, 78 of them carried AIDS and 65 of them had been genitally mutilated.
The forces that make people subject
girls to genital mutilation are varied. Sexual, religious, and sociological reasons are
often cited as causes. Some African
societies believe that the operation diminishes a women's sex drive. The decrease in
women's sex drive is sometimes ignorantly
believed to decrease the incidence of prostitution. Some religions, such as Islam,
advocate female circumcision. In some
parts of Nigeria, circumcision is a rank of
honour and distinction for both the girl
and the family. In Egypt, for example, the
uncircumcised girl is called 'Nigsa'
(unclean). Western efforts to eliminate the
practice through missionaries or colonial
masters have forced people to hold on to
their cultural traditions for fear of being
exposed to the ill effects of Western
society.
The most extreme form of female
circumcision, infibulation, is the complete
removal of the vulva! tissue including clitoris and the labia. After the tissue has
been removed, the sides of the wound are
sewn together. This leaves a miniscule
opening about the size of a matchstick. No
anaesthetic is used and the instruments are
not sterilized. [editor's note: Female circumcision can be done in groups, therefore
the sterilization of instruments is essential
in preventing the transmission of AIDS.]
Essentially, sexual intercourse is impossible
unless the vagina is reopened. This is often
done through forcible entry by the husband, which can lead to hemorrhaging. In
women, "infibulation is associated not only
with chronic pain, but with lesions in the
vaginal tissue which lead to the presence of
blood during intercourse," says Linke. He
further states that "it is noteworthy that
the recent outbreak of AIDS in Africa
corresponds geographically to those regions
in which female genital mutilation is still
practiced." We, at the women's centre, are
extremely concerned about the rampant
spread of AIDS and its connection with
female genital mutilation. We have
launched an educational campaign to
inform women about the situation by home
visits, newsletters, and public speaking
events. As a non-governmental voluntary
organization without a solid financial base,
the greatest problem in our ongoing campaign is funding. Any donations would be
greatly appreciated. Please help us to stop
female genital mutilation and the spread of
AIDS among African women. □
(From the International Symposium on AIDS in Africa,
Naples, Italy, October 7-9, 1987. )
Uganda:
1983 I 7 AIDS-cases
1987 I, 138 AIDS-cases
1987 6% of prostitutes are HIV-positive
Rwanda:
1981 10 AIDS-cases
1987 705 AIDS-cases, (246 are children)
Zaire:
I 987 6-8% of pregnant women are HIV-positive
1987 I 1% of prostitutes are HIV-positive
Congo:
1987 583 AIDS-cases
Kenya:
I 985 6 I% of prostitutes are HIV-positive
Tanzania:
198 7 1130 AIDS-cases
Cameroun:
1987 1.5% of pregnant women are HIV-positive
Ghana:
198 7 96 AIDS-cases
Senegal:
1987 14% of prostitutes are HIV-2-positive
Guinea-Bissau:
1987 60% of prostitutes are HIV-2 positive
Tunisia:
I 98 7 11 AIDS-cases
Contact:
• Ministry of Health
P.O. Box 30016,
Nairobi, Kenya
Further Reading:
• Report on AIDS, by the Panos Institute, 8 Alfred
Place, London, WClE 7EB, UK.
• The Politics of AIDS, 1he New Internationalist,
No. 169, March 1987.
• AIDS Acti on, (International newsletter fo r AIDS
info rmation), Published by AHRTAG, 85 Marylebone
High Street, London, WIM JDE, UK.
Contact:
• Hannah Edemikpong, Women's Center,
P.O. Box 185, Eket, Cross River State,
Nigeria, West Africa.
Further Reading:
• The Circumcision of Women, By O/ayinka Koso-Th omas, Z ed Books Ltd. , London 1987.
Connexions 25 Winter 1987
17
India
Cooking Inside
-The Effect of Wood Smoke on the Health of Women
(Excerpted from an article by Anil Agarwal
in Manushi, an Indian feminist monthly,
no. 28, 1985.)
Atmospheric pollution has long been
regarded as probably the least important of
all the environmental problems in rural
areas, a problem which is concentrated
mainly in major cities and industrial
towns. But recent evidence shows that air
pollution within homes may be an acute
problem, an underlying cause of millions of
deaths every year. The burning of cooking
fuel envelops the indoor environment with
heavy smoke, and women, who have to do
all the family cooking, may be daily
exposed to more pollutants than even
industrial workers in extremely polluted
environments on smoggy days.
For thousands of years, people have
cooked using firewood and cow dung.
Even today, over 90 percent of households
use wood, dung and crop residues as fuels.
Environmental protection agencies in
developed countries commissioned a
number of studies to assess the impact of
firewood use on air pollution. These studies revealed that biomass fuels, particularly in small scale combustion as in
residential stoves, emit several important
pollutants in high quantities compared to
gas, oil, and even coal-the most polluting
fossil fuel.
18
Connexions 25 Winter 1987
But what about homes in a country
like India where cooking is commonly done
on open and inefficient chu/has with few
arrangements to funnel the smoke out of
the house? A pilot study in four villages of
Gujarat was carried out in late 1981. The
woman cook in each household was asked
to wear a sophisticated air sampler which
was clamped to the collar, so that the
measurement device could move around
with the cook and measure her actual exposure to major pollutants in wood smoke.
The results were shocking. The average exposure of women to the pollutants
was over fifty times greater than the safety
levels set by the World Health Organisation. Women cooks receive a larger total
dose than would residents of the dirtiest
urban environment. Even an industrial
worker would rarely be exposed to the levels found in the Gujarat study.
A number of factors make the level
of exposure to pollutants worse. Dwellings
in villages are small and badly ventilated.
In one of the Gujarat households, when the
holes in the roof were closed, as is done
regularly in monsoon conditions, ventilation was so reduced that it became impossible for the researchers to remain in the
kitchen for more than a few seconds
because of the discomfort caused by heavy
smoke. The woman cook, however, stated
that such conditions were normal during
the monsoon.
What does this mean for the health
of women who cook? The most powerful
evidence for the ill effects of wood smoke
comes from a survey of a heart disease
called cor pulmonale, in which the right
lower chamber of the heart enlarges and
fails because of a disorder in the lungs. The
survey was carried out over a period of 15
years on hospital patients in Delhi. The
authors, Dr. S. Padmavati and Dr. S.
Arora, concluded that because of the fact
that women are exposed to smoky primitive fireplaces from early ages, domestic air
pollution accounts for the higher prevalence of cor pulmonale in women than in
men.
In Ahmedabad, another study of the
incidence of cough, cough with expectoration, dyspnoea (difficulty in breathing) and
lung abnormalities, found a statistically
higher incidence among women cooking
with smoky fuels. Furthermore, studies in
Nepal have shown a strong association of
domestic smoke with chronic bronchitis.
Exposure to carbon monoxide (CO),
a colourless and odourless gas which is
highly toxic if inhaled in sufficient quantities, is also a health problem for Indian
women. Evidence points to a strong link
between chronic CO exposures and both
heart disease and impaired fetal development. Recent evidence points to a strong
association of CO with heart diseases.
Any condition which results m
reducing the blood's capability to carry
oxygen to the tissues, like anaemia, will
also make a person more susceptible to carbon monoxide toxicity. This is particularly
bad for Indian women, who are anaemic in
large numbers. Chronic lung diseases will
further reduce the capability of the blood
to rid itself of carbon monoxide during
periods of low or no exposure. There are
several factors that make women particularly susceptible to CO exposure. Women
generally have less haemoglobin reserve
than men, which makes them more prone
to anaemia, and also makes them more
vulnerable to lower doses of CO than men.
During pregnancy, there is additional
demand on haemoglobin, further lowering
their reserves and making them even more
sensitive to CO. This exposure can also
affect the unborn child, leading to reduced
birth weight and increased perinatal death
rates. It is not surprising that respiratory
diseases are a leading cause of death among
women and girls over the age of five in
India.
Women begin cooking as young girls
and continue for much of their lives.
Young girls may receive significant exposure at their mothers' sides even before the
often tender age at which they begin cooking full time. In the case of cooking smoke,
inhalation is inevitable because exposure to
smoke comes with every breath. Pregnant
and nursing mothers generally have no
option but to cook and so remain exposed
to smoke.
There is general agreement that the
health of rural women is significantly worse
than that of the rural male population. A
number of reasons have been presented to
explain this phenomenon: high fertility
rates, less access to health care, inadequate
diets, and differences in economic roles.
Smoke exposure could also be one of the
major factors.
There are many steps to be taken
that will cut down the exposure to smoke
and reduce its adverse impact on women's
health. One aspect of the wood smoke
solution is to increase ventilation in the
homes of the poor. Ventilation improvement could be the least expensive, shortterm way to reduce smoke exposure.
Unfortunately, house designs are usually
decided by the males in the house who do
not spend endless hours cooking under
these horrid conditions. In addition, certain species of trees known to give off less
smoke when burnt should be grown in special forestry programmes.
Improved stoves are also a key factor
in solving the problem. The new Nada
stove, which former architect Madhu Sarin
helped to pioneer, evolved spontaneously
out of the traditional stove in the village
when Sarin worked closely with the stove
users. Sarin works closely with the
beneficiaries of the new technology, even at
the design stage. For Sarin, involvement of
women in stove dissemination programmes
is crucial. She argues that women seldom
make decisions even about their own technological needs and the little cash that
would be needed to purchase new technologies is denied to them by men. Thus, stove
dissemination programmes must be undertaken in a way that they support and
increase the confidence of rural women.
Sarin is today the most successful disseminator of improved stoves in India.
There are serious implications for
health policy planners in these findings.
Just as supply of clean water is now considered an extremely important domestic
need in the rural areas, the supply of clean
air is also a matter of high priority for
rural women. D
Further Reading:
• Looking at Appropriate Technology,
Women's World, an Isis International publication, Geneva, Switzerland, June 1986.
Connexions 25 Winter 1987
19
The earth's population is now over
five billion. The majority of these people
live in developing countries where the quality of the water supply and sanitation is
poor. The World Health Organization estimates that 80 percent of human sickness
and disease in developing countries is
related to inadequate water supply and poor
sanitation. The United Nations therefore
declared that the decade of the 1980s would
be devoted to providing these countries with
adequate water supply and sanitation.
Where water quality and sanitation
are problematic, women are greatly affected.
Some Third World women expend up to 27
percent of their caloric intake through the
heavy work involved in transporting water.
This work causes more than fatigue-pelvic
disorders and complications at childbirth
are often a result. In addition, mothers must
contend with the fact that children are
disproportionately the victims of water- and
sanitation-related diseases. For example,
water-borne diarrhoea illnesses kill over five
million children in developing countries
each year. Other water-related illnesses,
such as parasite worms and cholera, also
claim many children's lives. Because of
women's special role with regard to water
supply and sanitation, it is imperative that
women be actively involved in all aspects of
planning and implementing water projects.
20 Connexions 25 Winter 1987
Kenya
Water:
An Obstacle for African Women
(Excerpted from a talk by and subsequent
interview with Bibi Hamisi, an extension
worker with the Kenya Water for Health
Organization and Hilda Paqui, a United
Nations Development Program Information Officer from Uganda. Recorded for
Connexions on Nov 2, 1987.)
Q: How has the Water Decade affected the
world population?
Hilda: Due to efforts associated with the
Water Decade, 345 million people have
gained access to clean drinking water and
about 170 million have gained access to
better ways of disposing of their waste products. But because of population growth,
the number of people without access to
clean drinking water at the end of 1985
was the same as in 1979; so we have hardly
made a dent. Without the projects of the
water decade though, the situation would
obviously be much worse.
Q: Besides population growth, what are the
other factors which negatively affect water
supplies and sanitation?
Hilda: Shifting populations, for one; due to
migration, fifty percent of the Third World
population will soon be living in urban
slums. While water and sanitation are often
poor in rural areas, it is even more difficult
to find solutions for people living in urban
slums and squatter settlements.
Q: What role do women play in this
scenario?
Hilda: In 1986, the United Nations
resolved that attaining self-sufficiency with
regard to food is a top priority in order to
help Africa eliminate its current economic
bind. In Africa, women are responsible for
80% of the food production. Therefore,
unless we release women's time and energy,
this goal cannot be achieved. In rural
Africa, women must put forth tremendous
efforts in order to obtain water. For
instance, in Burkina Faso during the dry
season, women walk to distant water
sources after sunset, sleep there, and then
return at dawn carrying 25 kilos of water.
You can imagine how physically exhausted
a woman must feel after spending at least
seven hours collecting water and also after
having slept outside. She will have little
energy to work in the garden, grow and
process food, take care of her family, or
generate income. She certainly won't have
time to take care of herself. It is also
important to train women in agricultural
methods and to obtain better seeds and
farming tools (for which financial credit is
necessary). But time and energy is the most
crucial factor in African women's lives. If
they do not have the time, they cannot take
advantage of training and improved farming equipment.
Q: In which project are you involved?
Bibi: We train women to maintain newly
installed, hand-operated water pumps. My
major role in this project is to train and
mobilize the community.
how to make deposits and withdrawals
from their banks. Then we hold workshops
to train the women in water pump maintenance. After the women learn how to
assemble and dismantle the pumps, they
get a chance to practice out in the fields
and to train other women to maintain the
pumps. We do follow-ups to see how they
are doing. If they are successful, we finally
provide them with a pump. So far, we have
provided pumps for fourteen communities,
and they are being run well.
Q: How did this project get started?
Bibi: Before the water pumps were
installed, women had many health problems. Women had to walk four or five
kilometers away from home in search of
water. The little water they do find is often
contaminated. In 1979, we had an outbreak of cholera. The situation was so bad
that in 1983 the Ministry of Water
Development came up with a plan for providing clean water to help communities
control such diseases; the Ministry drills
boreholes and we mobilize and train the
community. The real challenge of providing villages with water does not lie in drilling wells and installing pumps, but in
making sure that the pumps continue to
work properly. The community must be
trained to do preventive maintenance and
to properly care for the pumps, if the project is to be successful.
Q: How do you involve local communities?
Bibi: Before a drilling, community
members consult with us about the water
availability in their area. After that, we do
a household survey to find out how many
permanent residents there are in that area.
There should be a well and a pump for
every 125 residents. Otherwise, they will
break frequently from overuse. Then, the
community members form water committees whose purpose is to make suggested
improvements about the project. We
require the community members to contribute money to the project in proportion to
their incomes. They get together to discuss
how much to contribute either on a daily,
weekly or monthly basis. They also select a
secretary, a treasurer and a chairperson,
who are in charge of financial matters.
These three people are usually women, particularly the treasurers. We show them
UNICEF/Bernard Pierre Wolff
Connexions 25 Winter 1987
2I
Q: What has led you to give priority to
training women?
Bibi: The men are not trustworthy. We had
a lot of problems when men took care of
the money. For example, in one community we suggested that they get a box in
which to store contributions. Although the
box could not be opened from the outside,
the men found ways to crack it open. That
was really upsetting! Our experience in
Kenya shows us that men are interested in
money more than anything else. Often
they care little about the welfare of their
own families. Sometimes families have to
live without husbands and fathers for
several months. We have found that it was
of no use to train men to look after pumps
because problems would occur, and the
man in charge would not be there to take
care of them. At one point, the men in the
community corriplained that we were
selfish; they wanted us to include more
men in the training. We did not want to
show them that we did not like them. We
have had to begin choosing one man for
each training session so that they would
feel recognized. Currently, one man and
five women maintain each pump.
Q: Who elects the maintenance workers?
Bibi: The communities do. We want them
to choose their own people because they
know who is good.
Hilda: When the villagers select women to
train for hand pump maintenance, there
are certain criteria they use. For example,
they might choose somebody who lives
closer to the well so that she can walk over
to the water pump with her children.
Q: Are you working with different women's
groups?
Bibi: Oh yes, we work with fundraising
groups. First, they register themselves, then
they find a way of generating some income.
Q: Have women's roles and status been
improved by their involvement in the
maintenance of the water pumps?
Bibi: Oh yes, of course, especially because
women now engage in income generating
activities. Some groups have even started
building shops for grinding machines. People walk ten to twenty kilometers to use
their grinding machines.
Hilda: When I visited Bibi's project two
years ago, another thing the women were
doing was growing vegetables around water
pumps-using run-off water. By doing so,
they can sell the vegetables and raise
money for pump maintenance and, in five
or ten years, pump replacement. Growing
and selling vegetables in the community
also helps improve community nutrition.
So water pumps have all kinds of spin-off
advantages.
Q: In what other ways has the installation
of water pumps affected the health of the
community?
Bibi: Well, cholera has been eradicated. We
have fewer cases of bilharzia. Malaria has
remained a problem because there is still
stagnant water-it is not spread by drinking
water. Diarrhoea is also less of a problem.
22
Connexions 25 Winter 1987
Q: What about sanitation?
Bibi: We are in the process of implementing a project that improves sanitation. The
Ministry of Health provides the labor, the
communities provide the construction
materials, and we coordinate the activities
of the Ministry and the communities. They
have started to construct pit latrines in
public areas, such as the health center,
mosques, schools, and markets; in some
villages groups of ten to thirty people are
digging pit latrines for every household.
We are trying to use local materials in the
construction of the latrines. Local materials are inexpensive. In addition, community members are involved in the construction; thus they have an investment and
they also acquire the expertise to maintain
the latrines properly. But most importantly,
this project, like the provision of water
pumps, is improving the health and well
being of the women of Kenya. □
Contact:
• International Drinking Water Supply
and Sanitation Decade, Hilda Rwabazaire
Paqui, United Nations Development Programme, Room DCl-1902, One UN Plaza,
New York, NY, 10017.
Further Reading:
• "Women and Water," Women's World,
an Isis International publication, Geneva,
Switzerland, June 1986.
• "Water Well," Connexions #6, Fall 1982.
• "Women, Water, and Donkey Work,
Kenya," Women's World, an Isis International publication, Geneva, Switzerland,
December 1986.
Canada
Women and Substance Abuse
(Translated from an article by Marie-Claire
Dumas in La Vie en Rose, • a Canadian
feminist monthly, October 1986.)
Two hundred women gathered at a
1986 conference entitled "Women and
Drug Addiction" in a town north of
Toronto, Ontario. Women addicts and exaddicts themselves were the main participants. Most of these women were searching
for help-not only with their addictions,
but also with the pain that has in so many
cases been responsible for the onset of their
addictions. All kinds of drug abuses were
addressed, from heroin and cocaine to
tobacco and alcohol.
Alcoholism is now having a profound
effect on young women, single women, and
women who live and work in large cities.
For these women, alcohol works as a
mechanism to help relieve the stress that
comes
when
they
don't
receive
"compensation-financial, psychological, or
social-that is their due." Women who are
especially at risk are those working in jobs
that are menial, repetitive, and low-paying.
They face constant battles against low selfesteem and the frustration that comes from
doing monotonous work. Since these
women have little or no support network,
their negative feelings can be repressed, at
least temporarily, by drinking alcohol.
Unfortunately, alcoholism in Canada is the
third leading cause of death among women
ages 33 to 55 (Women's Health).
The other "legal" addiction which is
having a devastating effect on the women's
community is tobacco addiction. Cigarette
smoking has been increasing among women
since the 1960s. In contrast to previous
studies, it is now reported that in the 12 to
19 age group there are more girls smoking
(25 percent) than boys (20 percent). There
are many factors which can account for
this historical change. Studies have shown
that cigarette smoking is associated with
the repression of negative emotions such as
anger and anxiety. Unfortunately, women
are often discouraged from expressing these
negative emotions, and then turn to
cigarettes for a release from frustration. In
addition, ever since the late 1960s,
cigarette smoking has been commercialized
as an empowering tool-a habit which
signifies women's equality with men. The
tobacco industry portrays women smokers
as self-assured, strong, and confident. But
what the tobacco industry does not tell us
is that women in Canada are dying in
record numbers from lung cancer and other
diseases caused by cigarette smoking.
Women must pay particular attention to the risks of drug addiction, says
Louise Nadeau, a toxicologist at the
University of Montreal. She believes that
women are more at risk because of the
nature of women's role in society. The
characteristics of the feminine role-selfsacrifice and subservience to others-have
brought about a feeling of loss of control
over the environment. This loss, she says,
"plays an important role in the distress so
uniquely felt by women, a distress manifested in certain cases by depression, anxiety, and the use of mood-altering drugs."
Another factor which often plays a
part in women's addictions to drugs is sexual abuse. Statistics indicate that violence
and sexual abuse have been part of the
lives of at least 70 percent of Canadian
women who abuse drugs. Most women at
the Canadian conference felt that 80 to 90
percent are more accurate figures as many
cases of sexual abuse go unreported.
What are the best ways to help these
women break their cycle of addiction?
Many individual treatments were discussed, but the participants agreed that in
order to be effective, any approach must be
comprehensive. A group in Southwest
Ontario, The Women Being Well Project,
says that the approach must be positive,
but holistic. No treatment program is likely
to work unless the causes of the addiction,
as well as the addiction itself are treated.
Detoxification must include treatment of
past sexual abuse and must be tailored to
meet the individual needs of the women it
serves.
The problems associated with drug
abuse are particularly poignant for women
of color. Maggie Hodgson explains the toll
that alcoholism takes on families of color,
"It is easy to understand why the tolls of
alcoholism are so high when one examines
the degree of personal and collective
misery that are ours." Drug addiction
treatment centers which cater to white
women often cannot address the issues of
concern to women of color; consequently
the treatments are ineffective. Ms. Hodgson
explains what has been done to meet the
needs of women of color: "We have formed
our own program called Nechi (translation:
my soul touches yours). Between 60 and 80
percent of our participants are survivors of
sexual abuse."
Ms. Hodgson espouses a philosophy
of healing that all women would do well to
remember: "We reclaim our spiritual
center and we work in concentric circles
towards the family, our women friends, our
community, and towards political action."
Further Reading:
• "Tranquility Can Kill," by Linda Rauch
Peregal,
Healthsharing,
a
Canadian
Women's Health Quarterly, Winter 1982.
• "The Politics of Quitting Smoking," by
Patricia Rawson and Debbie Holmberg
Schwartz, Herizons, a Canadian women's
news magazine, December 1984.
Connexions 25 Winter 1987 23
Together
We
Switzerland/Nicaragua
(Excerpted from "Support through SelfHelp" in Women's World, an Isis International publication, no. 8, December 1985,
and "Internationale Kontakte des FFGZ"
in Clio, a West German feminist self-help
magazine, no. 26, March 1987.)
The Dispensaire des Femmes in
Geneva is an autonomous women's health
center set up in 1978. The sixteen women
of the Dispensaire work as a collective.
The aim of the center is to provide preventive health care and information and to
help women gain better control over their
own bodies and health. They do research
into and provide alternative treatment,
including
naturopathy,
acupuncture,
homeopathy, and nutrition. One of the
members of the collective, Rina Nissim,
has written a highly successful book on
natural healing in gynecology. On visits to
Nicaragua, Nissim established contacts
with various women's groups there.
Many women in Nicaragua are illinformed about their bodies and their fertility. A study conducted at the Berta Calderon maternity clinic in Managua showed
that 10% of the women who had an illegal
abortion died of the ensuing complications,
and that another 25% remained permanently sterile as a result of abortionrelated infections. Nicaraguan women are
working toward reform of the law that
declares abortion illegal, and they are trying to make information on contraception
and sexuality more readily available. They
asked the women from the Geneva Health
Collective to share their experience and
knowledge with Nicaraguan women.
The women from Switzerland and
Nicaragua decided to collaborate on a
health project. They traveled around the
country in a car equipped with informational material, specula, diaphragms, gel,
surgical utensils, gauze, etc. During the
summer of 1987, this "mobile women's
health center" visited various women's
groups in Nicaragua in order to acquaint
women with basic knowledge about health
and contraception and to support them in
their demand for self-help.
This movable project makes it possible to transmit knowledge from one selfhelp group to another in spite of limited
resources. Through the travel of one
woman equipped with the necessary
materials, many women can be reached.
24
Connexions 25 Winter 1987
Are
Piers Cavendish/Reflex
Mauritius
"Disease NO-Health-YES: A Medical Manual," is a booklet published by four
progressive Mauritian organizations: the
Bambous Health Project, the daily LAUT,
the Women's Liberation Movement, and
the literacy program "Education for Work"
in 1986. The literacy program, which compiled, printed and distributed the booklet,
also used it in their courses. The booklet,
written in Creole (which is spoken by 52
percent of the population), explains in an
accurate and accessible manner how local
diseases come about, how to to cure them,
and most importantly, how to prevent
them. It covers a range of illnesses including amoeba-related illness, appendicitis and
AIDS. With regard to the latter, the
manual stresses the fact that anvone, not
just male homosexuals, can be affected by
the disease.
The Bambous Health Project is a
cooperative founded in May 1975. An executive committee takes care of organizational tasks. The project employs a fulltime doctor and 350 families participate.
In 1978, a pharmacy with all essential
medicines was set up. In addition, a oneyear training course for health volunteers
was instituted. The course trains villagers
in basic knowledge of health and hygiene
in order to break the monopoly of the medical profession-once they go back to their
village they organize their fellow villagers
to eradicate various diseases. The courses
are taught in Creole. The syllabus
comprises functions of the body, first aid,
nutrition, occupational disease, women's
diseases, contraception, pregnancy, alternative care and preventive medicine. According to the manual, 25%-35% of all diseases
could be prevented. The Bambous Health
Project considers itself an alternative to
both the private medical establishment and
the National Health Service. Private medicine is prohibitively expensive, and statecontrolled health care is afflicted with
bureaucratic control, corruption and political favoritism.
Strong
Bangladesh
(Translated from "International Contacts
of the FFGZ" in Clio, a West German
feminist self-help magazine, no. 26, March
1987.)
In 1976, Rokeya Begum founded a
women's self-help project called "Self Reliance Development Society" in Netrakona,
Bangladesh for women from the nearby
slums. Over the course of seven years of
organizing and lobbying, Rokeya gained
the support of the better-off women in
Netrakona. She even received a government credit of $US 5000. With this money,
she built a small building to house the project and bought two sewing machines, a
knitting machine and an embroidery
machine. Seventy women found paid jobs
in the project. They manufactured clothes
and batiks, sisal wall hangings, bamboo
furniture, etc. Soon afterwards the project
was expanded. A day care center for children from the slums was set up-the children receive milk at the center once a
week. The center offers courses on healthrelated issues and contraception as well as
basic literacy programs. The demand has
been so high that the women can only work
for a few hours at a time; they have to
alternate and many women cannot even be
admitted.
The center has often been the target
of state control; it was shut down several
times for political reasons. In 1985, the
machines were confiscated because the
women refused to have their project turned
into a propaganda instrument of the
government. In 1986, the women had to
start again from scratch. Rokeya and other
women worked tirelessly on the reconstruction of the center. The women have started
to work there again, and they plan on setting up a small women's health center.
Monique Jacot/Dispensaire des Femmes/ISIS
Berlin
(Translated and excerpted from "Feministische Selbsthilfe und Gesundheitsarbeit im
Rahmen konservativer Sozialpolitik-Eine
Standortsbestimmung" in Clio, West German feminist self-help magazine, no. 23,
May 1985.)
The Feminist Women's Health Collective was founded in 1977. The Collective was organized as a politically
motivated self-help group. Our purpose is
to make sure that women become fully
acquainted with their bodies and become
responsible for their health. We encourage
women to work with other women to set
standards of health and sexuality. We also
want to reinforce the awareness that health
and disease are intimately related to the
overall living condition of women.
We work to provide this service for
little or no pay. We publicly demand that
women should not have to do any unpaid
labor, but have been unable to realize this
goal for ourselves. As an autonomous project, we depend on income generated by
the Collective and on donations. Most of
us must have other income in order to pay
our bills. But we do find that working to
better women's lives is very satisfying and
meaningful work.
Our services at the health collective
help to balance the deficits of the statecontrolled health system. We have always
considered our work not only a reaction to
existing shortcomings or a correction of
gaps in the state-controlled health system,
but also a necessity in the movement
toward control by women of their own
bodies. We did not expect financial assistance from the government, as we believed
that self-determination for women could
only take place in an autonomous group.
We deliberately disassociated ourselves
from traditional patriarchal institutions
such as the government health care system.
Ironically, that same system has recently
begun to praise the women's self-help
movement. The government intends to
reduce state-sponsored care to a supplemental resource and eventually plans to
abolish it altogether.
The government's new alliance with
the alternative health movement is highly
suspicious.
Conservative
government
officials have finally assessed the economic
value of the alternative projects-they conceive of the services as an effective means
to save government money. During the
recent economic crisis, many women were
laid off. The unemployment rate among
women doubled from the years 1981 to
1983. Instead of having paid jobs, women
were expected to perform some form of
social work. Ultimately, this means that the
government is unjustly making money off
of women's unpaid labor.
The budget for social services has
been cut and self-help groups are suddenly
deemed important in supplementing state
services. How does this translate into daily
politics? While the state-run hospitals in
Berlin cut two thousand jobs (which saves
the state 100 million DM), state agencies
encouraged private non-profit organizations
to create 467 jobs for social workers (which
costs the state 5.2 million). The pseudoprogressive rhetoric surrounding these drastic measures suggests that social services
are being qualitatively improved, whereas
in actual fact the measures represent
regressive social politics implemented
mainly at the expense of women.
In June 1982, women's and alternative projects were supposed to receive 10
million DM. In the fiscal year 1983, this
amount had shrunk to 7.5 million, and was
further decreased in 1984 to 6.5 million.
Only half of these monies were directly
allocated to various projects; the other half
mysteriously disappeared into the state
bureaucracy. Moreover, the intention was
by no means to gradually provide salaries
to more self-help workers, but to allocate
just enough money for a part-time or a
full-time position; one of the main functions of the recipient of that job was to
mobilize and organize volunteers. The
privatization of public services is presented
as a solution to social problems, but in
essence, current social politics will result in
the exploitation of self-help health workers.
Further Reading:
• CLIO, a West German feminist self-help
magazine, FFGZ, Bambergerstr. 51, 1000
Berlin 30 (West).
Natural Healing in
Gynecology, A Manual for Women, by
Rina Nissim, R outledge and Kegan Paul,
London 1986.
Clio
c:IOC: DC1011rr1' ZCIIS(nrlll
zur SCIDllnllFC:
26
WOMEN IN THE BAY AREA
We need more volunteers to help with upcoming issues. If you are interested in working on
our project, have language, editing, layout or fundraising skills, we'd like to hear from you.
See our address on the inside back cover.
Connexions 25 Winter 1987
25
Shorts
Canada
(From the proceedings of the Coalition of
Provincial
Organizations
of
the
Handicapped's Workshop on Disabled
Women's
Issues;
edited
by
April
D' Aublin/Research Analyst; March 1987,
Reproductive Rights Workshop by Maria
Barile.)
I want to make it clear that when I
talk about "choice," I am talking about
choice in all areas-the choice to have children, to have an abortion, or to adopt children.
The reproductive rights of women
involve four areas. All women must be free
to prevent and end unwanted pregnancies
regardless of their economic means.
"Reproductive rights" also implies that
women should be able to choose if, when
and how to have children. This means that
no woman should be forced into abortion
or sterilization, or to risk infertility due to
dangerous birth control methods such as
Depo Provera and the Dalkon Shield.
Disabled women in particular are
discriminated against with respect to reproductive rights. Many people believe that
disabled women are psychologically incapable of conceiving and bearing childrenthat disabled women must decide not to
have children. From a very early age,
women are made to feel that they have a
responsibility to produce healthy childrena disabled child is seen as a woman's
failure. Because some disabled women have
a greater chance of having a disabled child,
disabled women are often coerced into
unwanted abortion and sterilization. In
addition, disabled women are often sterilized without first having been given the
facts about the procedures involved.
If a disabled woman chooses to have
children, then the questions arise: Who will
care for the infant? Who will pay for extra
help or specialized technical aids? When it
comes down to it, it is a socio-economic
question that our able-bodied sisters do not
need to consider. A disabled women is
always made to feel that the choice is not
hers and her partner's but that of the state.
On the question of abortion, disabled
women share with every other woman the
concern for safe and economical abortion.
Most often disabled women, unlike ablebodied women, are encouraged to have
abortions when they become pregnant,
even if they are pregnant by choice. The
Office of the Handicapped does not have
any plan for dealing with childbirth or children. Disabled women are also able to get
an abortion more easily than most other
women. Now I don't mean to sound prolife, but our private choice is limited
because we are disabled.
There is another problem that comes
with reproductive "choice". Through
amniocentesis, women are now able to find
out if their fetus is disabled. Women can
then abort the fetus if they choose. It is a
responsibility of those of us who have lived
as disabled people to make sure that
women find out that it is O.K. to live as a
disabled person, and that we have good
lives regardless of our disabilities.
Switzerland
'.'j
-,,,
"c:,
!:=
.~
(Submitted by Elizabeth Ferris, World
Council of Churches, Geneva, Switzerland,
November 1987.)
c::i
~
26 Connexions 25 Winter 1987
~
~
:i:;
§
"I had the feeling that I was dirtying
the boat by my mere presence. The others
left me more room-either out of pity or
because I was 'dirtier' than they were. I
was glad if they avoided looking at me."
These words, spoken by a Vietnamese
refugee about her rape by pirates, convey
some of the pain that many women
refugees face during flight. Although this
young woman received medical care and
counseling when she arrived in Pulau
Budong, Malaysia, the physical and emotional consequences will last for many
years. The many victims of pirate attacks
are but one example of the violence that
many refugee women face during their
flight to safety. The violence takes many
forms: from abuse at European airports to
forced prostitution along the Mexican
border to sexual exploitation by border
guards in Djibouti. The scars of violence
run deep, leading to physical and emotional trauma-trauma compounded by the
experiences of exile.
It is difficult to generalize about the
world's 15 million refugees. But, most
refugees around the globe are women and
girls and they do face particular health
problems. Like all refugees, women often
cross borders in a state of exhaustion.
Some have experienced pursuit, others
have walked for days with little food or
water. For refugees arriving in camps or
settlements, often times there are inadequate water supplies and poor sanitation
facilities. These conditions are conducive
to breeding many diseases-refugees are
particularly susceptible because of their
poor physical state upon arrival. Women
often experience malnutrition especially
when they are pregnant or breast-feeding.
Also, if the food supply is limited, mothers
may neglect their own needs in order to
feed their children first.
But along with the physical conditions, other factors, less understood by
relief officials, influence the health of
refugee women. Women are the traditional
guardians of culture and are often the ones
trusted with keeping families together.
Because of this, refugee women feel
disoriented by having their culture
uprooted and families separated-they are
unsure of their role in the new environment.
Although the vast majority of the
world's 15 million refugees are women,
health services are not set up to meet their
netids in many countries. As a woman
working with Ethiopian refugees explains,
"because the women are responsible for
collecting fuel and water and for taking the
children to health care and feeding programs, they are the last to receive health
care. When the out-patient department was
finally set up, men made up 67 percent of
the patients. The women did not have the
time." For Moslem refugees, cultural factors also limit women's access to health
care. In Pakistan, for example, most of the
2-1/2 million Afghan refugees are women
and girls. Yet, they can receive medical
treatment only from women doctors, who
are in woefully short supply. This contributes to further malnutrition and disease.
Refugee women not only have serious health needs, but also have an important role to play in preventing disease, promoting nutrition, and in educating the
community about the importance of safe
water. Their knowledge and experience in
traditional medicine is a resource to be
used by the community. Refugee women
must continue to demand a greater role in
making the decisions that affect their
health and the health of their children.
Malaysia
(From Women in Action, an Isis International publication, Supp. n.6, December
1986.)
The Malaysia-based Third World
Network has issued an urgent call for
action to pressure the World Health Organization to reverse a policy decision on
breastmilk substitutes for newborn children. The policy threatens to undo some of
the hard-won gains of the decade-long,
worldwide campaign by women's and consumer advocates groups to limit multinational corporations' promotion and marketing of breastmilk substitutes, particularly in
developing countries.
The policy came as a result of a
request by many countries for guidelines
clarifying the intent of the International
Code on the Marketing of Breastmilk Substitutes, a model code for national legislation adopted by the World Health Organization in 1981 for limiting the marketing
and promotion of bottled milk products.
Though grassroots groups consider the code
a crucial victory in the struggle to protect
breastfeeding from unfair commercial competition, one criticism they have raised all
along is that the code still leaves sizable
loopholes for infant formula companies.
pients of free or subsidized supplies of
breastmilk substitutes. (One gaping loophole in the Code has permitted infant formula companies to continue giving large
amounts of free milk supplies to hospitals
and clinics.) However, this crucial provision was omitted from the final guidelines
published by the World Health Organization in May 1986.' Anonymous sources
inside WHO admitted to the daily newspaper International Herald Tribune that the
provision was omitted because of pressure
from the United States and baby food
manufacturers.
The development represents a blow
to the pro-breastmilk movement after so
many
years
of fighting
for
the
WHO/UNICEF International Code and
launching a highly successful campaign
against the Nestle corporation, one of the
major infant formula companies.
The Third World Network asks individuals and groups to write letters expressing their concern over the matter and urging the agencies to reinstate the provision
regarding free supplies.
Contact:
• Third World Network,
87 Cantonment Road,
Penang, Malaysia
New Zealand
(From Women in . Action, an Isis International publication, Supp. no. 6, December
1986.)
lfiEles
-artifici&I iff\i tat\On
BKBY Ft>OD
Partly for this reason, health and policy experts from eight countries met with
WHO and UNICEF staff in December
1985 to draft guidelines for implementing
the code. One of the most important provisions they agreed upon was that maternity
wards and hospitals should not be the reci-
The New Zealand Women's Health
Network is a national network of feminists
concerned about health. The group, created
ten years ago, aims to provide a forum for
women, especially non-health professionals,
to discuss and educate one another on
health problems and develop responses to
local and national health policies. The network defines health in the broadest sense,
encompassing social and economic issues
such as alcohol abuse, disabled women's
sex problems, lesbian motherhood, incest,
industrial health, and patient's rights.
The group carries out a series of regular activities, including publishing a
bimonthly newsletter, organizing occasional
conferences and workshops, and distributing resources such as a friendly and accessible booklet Coping with Menstruation:
Information for Disabled Women. Besides
dealing with the concerns of disabled
women, the group's publications and programs also focus on the health situation
and needs of the islands' indigenous Maori
women. Finally, the network puts New
Zealand women's health groups in touch
with women's health groups in other countries.
Contact:
• New Zealand Women's Health Network,
P.O. Box 2312,
Tauranga, New Zealand.
Connexions 25 Winter 1987 27
(cont. from p. 11)
HELAINE VICTORIA PRESS
little tolerance for abnormalities, diseases and disabilities. I think
the motivation behind this intolerance is related to the desire to
keep a " superior" gene pool in German society-a desire which
has a historical base in eugenic actions taken by the Nazis.
In fact, research indicates that many of the women who
were sterilized by Nazi orders led lives that today we would call
" feminist." In the special Nazi courts that dealt with forced
sterilization, these feminist women were labeled "socially disabled" and therefore candidates for sterilization. It is very frightening to see that involuntary sterilization of women continues in
West Germany. But now the issue is being debated with a historical perspective that I hope will motivate people to eliminate the
attack on disabled women's reproductive rights. □
A SMALL FEMINIST
PRESS SPECIALIZING IN
WOMEN 'S HISTORY
POSTCARDS FOR OVER
14 YEARS.
~~
Important & dynamic
photos on the front &
biographical capti o ns
on the back .
Contact:
• Theresia Degener
2318 Parker #A
Berkeley, CA 94704
or
Prozessionsweg 8
4417 Altenberge, Federal
Republic of Germany
• Anneliese Mayer
C/O AG SPAK
KISTLERSTR. l
8000 Munchen 90
Federal Republic of
Germany
• Judy Heumann
World Institute of Disability
l 720 Oregon Street #4
Berkeley, CA 94703
Further Reading:
• With the Power of Each Breath, A Disabled Women's Anthology, Edited by Susan E. Browne, Debra Connors, and Nanci
Stern, Cleis Press, Pittsburg, PA, 1985.
• Geschlecht: Behindert, Besondered Merkmal, Frau, (A book by
and about disabled women), C. Ewinkel, G. Hermes, and others
(eds.), AG SPAK M68, Munchen, 1985.
• Kruppel-Tribunal, Menschenrechtsverletzungen im Sozialstaat,
(A book about violations of disabled peoples rights), Edited by
Susanne V Daniels, Theresia Degener, Andreas Jurgens, Frajo
Krick, Peter Mand, Anneliese Meyer, Birgit Rothenberg, Gusti
Steiner, and Oliver Tolmein, AG SPAK, Munchen, 1983.
• "Das Bose Erbe," Emma, a West German feminist monthly,
November, 1984.
• "Die sollen-und die anderson durfen nicht," Emma, a West
German feminist monthly, August, 1985.
Special focus on
Black & Latin
American women,
U.S . Latinas , labor
history & other
topical material.
Madam C.J Walker, Black
millionaire & philanthropist
Send $1 . for catalog & 2 sample cards .
Helaine Victoria Press , Dept. Cx .,
411 E. 4th St. Bloomin ton , IN 47401
Qay
CWomett
For a change in your life we invite you to
,
try: The Wishing Well Magazine. Features
hundreds of current members' self-descriptions (by
Code #), letters, opinions, valuable resources, reviews,
and much more. Introductory copy $5.00 ppd. (mailed
discreetly first class). Confidential , supportive, dignified,
sensitive, prompt. Beautiful, tender, loving alternative
to "The Well of Loneliness." Fully personal, noncomputerized. Reliable reputation. Established 1974.
The pioneer of them all! Free information. Gay
women are writing and meeting EVERYWHERE
through:
en. r1 1 1 ,. r1 1 1_11n P.O. Box G
une ~wisnlttg ~w~\:'. Santee, CA 92071
I
BIG MOUNTAIN Help maintain s3cred lands at
Big Mountain . Inspiring new fullcolor poster with artwork by
Andrea Kay Smith. 25x32 . By
mail, $22 .50. Send $ 1 for fall '87
full-color catal og of posters,
cards and th e Carry It On Peace
Cal endar Wh olesale welcome.
VISA/ MC.
Pl4 580
SYRACUSE CULTURAL WORKERS, Box 6367, Syracuse, NY 13217 (315) 474-1132
28
Connexions 25 Winter 1987
rr- ~
~
Thank you so much! I think Connexions is wonderful-it helps to transcend
boundaries and barriers .. .! wish only the
best for the collective.
Sincerely,
Joanne M. Ursino
Ottawa, Ontario
Canada
Greetings! I received my very first
issue of Connexions on women in the
visual arts and needless to say, I've enjoyed
it tremendously! I am proud to be on the
Connexions mailing list. "Nakedness:
Movement and Confrontation" made me
realize that our bodies are such wonderful
works of art. Too bad one can't be seen
without all the negative additives.
The article on "Shared Moments
with Working Children" was great too
-very enlightening. It's a sad affair how little children are exploited.
The article "Agents of Change" was
like a breath of fresh air! Beautiful. This
article holds my ideal concept of progressive change. I personally feel that it would
be nearly impossible to convince many
men of the importance of women in our
society, but we can teach our sons and
daughters that men and women are of
equal worth. Perhaps if the same approach
that "Agents of Change" demonstrates is
utilized in our country, we might see progressive change happen in our lifetime. Oh
how I wish the feminist movement success
and pray for an awakening in the minds of
men.
In Solidarity,
Comrade Charles Logan
Jackson, Michigan
Gabriel's
apartments & guest rooms
for women & their friends
(617) 487-3232
104 Bradford Street
Provincetown, MA 02657
,,;:-__,_. ~--:-i \ "~':_:..i"~
Her eyes are miniature globes, in them there
is a country, one she visits while she
rocks and hopes the country disappears.
She sits on the cold shore, tugging her hair,
watching the clouds strain rain over the sea;
her eyes are miniature globes, in them there
is a country. That one she tried to tear
out of an eye. All day she watches, sleeps,
rocks and hopes the country disappears.
With )1er hands she covers her eye, the glare
of the sun deranges her diminutive dreams.
Her eyes are miniature globes, in them there
behind the rainstorms, into the blue air
yet it doesn't. She sits, waiting for weeks.
Her eyes are miniature globes in them thererocks and hopes; the country disappears.
J
ya -;-c .
•
Politics and Teaching
Do Mix
Feminist Teacher, a magazine
for teachers of all grade levels, in
traditional and nontraditional settings
• articles
• interviews
• bibliographies
• book reviews
• news and more
Feminist Teacher
Three times per year.
Ballantine 442
$12 U.S., $15 Canada (US Funds)
Indiana University
$16 outside North America
Bloomington, IN 47405
Name _______________________
Address _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __
Teaching interests, institutional affiliation:
Woman Waiting
are castles with rooms, but they are bare
Staring at the dark stones, she violently
rocks and hopes the country disappears
Gabriel Brooke, Innkeeper
Open Year Round
Cable TV & Coffee
Hot Tub & Sun Deck
In the Center of Town
(Submitted By Marisella Veiga, Santurce,
Puerto Rico)
ERRATA for VISUAL ARTS# 24
on p. 3-Doris Lotch should read Doris
Lotsch
on p. 25-par. 1: April 27, 1987 should read
April 27, 1986
on p. 26-GSMG+K should read GSMB&K
Gesellschaft Schweizer Malerinnen, Bildhauerinnen
&
Kunstgewerblerinnen
(member IAWA)
on p. 27-Centre Audiovisuel, Simone de
Beauvoir should read Centre Audiovisuel
Simone de Beauvoir
on p. 27-Christa Biedermann, artist should
read Christa Biedermann and Krista Beinstein, artists
on p. 27-Rahnuma Ahmed, artist should
read Rahnuma Ahmed, Nari Shongoti,
Dilara Begum Jolly (CONTRIBUTORS),
Center for Social Studies, Arts B1 Dhaka
University, Dhaka, Bangladesh
on p. 27-Jin Sook Kim, artist should read
Jin-suk Kim and In Sook Kim, artists
on p. 27-Duloe Maria Lopez Vega should
read Dulce Maria Lopez Vega
on the back cover, the caption and credit
should read "Witch" from the series
"Witch-Pictures," Krista Beinstein, camera
and Christa Biedermann, in front of camera
We apologize for any inconvenience our
inconsistencies may have caused.
Connexions 25 Winter 1987
29
Health Resources for Women
••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••
Argentina
Mabel Bianco, Coordinator of the Women, Health, and Development Program, Defensa l 20-4piso, of. 4080, ( 1345) Buenos
Aires, Argentina
Australia
Adelaide Women's Community Health Centre, 64 Pennington
Terrace, North Adelaide 5006, Australia
Leichhardt Women's Community Health Centre, 164 Flood
Street, Leichhardt, New South Wales, 2040, Australia
Liverpool Women's Health Centre, 273 George Street, Liverpool,
Australia
Austria
Osterr AIDS Hilfe, Lenaug. 17, A-1080, Vienna, Austria.
Bangladesh
Consumers' Association of Bangladesh, 32012A West Dhanmandi
Road, No. 8A, Dhanmandi RIA, Dhaka, Bangladesh
Belgium
Aimer d Louvain la Neuve, Cour des 3 Fontaines 31, 1348
Louvain la Neuve, Belgium
Brazil
Centro Informar;do Mu/her, (contact for further listings of
women's health groups in Brazil), Caixa Postal 11.399, 05499
Sao Paulo, SP, Brazil
Dominican Republic
Colectivo Mujeres y Salud, Apartado 22248, Santo Domingo,
D.N., Dominican Republic
France
Groupe Pratique Sante, 15 Rue J.B. Say, 69001 Lyon, France
Hong Kong
Asian Community Health Action Network, Flat 2A, 144 Prince
Edward Road, Kowloon, Hong Kong
India
Women's Centre, (information about amniocentesis and other
women's health issues), 104B Sunrise Apts. Nehru Rd., Vakola,
Santa Cruz (East), Bombay 400 055, India
Voluntary Health Association of India, C-14 Community Centre,
Safdarjung Development Aera, New Delhi 110 016, India
Rural Women's Health Group, Rural Development Society, 15/1
Periya Melamaiyur, Vallam Post, Chingleput 603002, South
India
Ireland
Dublin Well Woman Centre 73 Lower Leeson Street, Dublin 2,
Ireland
Ulster Cancer Foundation, 40/42 Eglantine Avenue, Belfast BT9
6DX, Northern Ireland
Defend the Clinics Campaign, National Committee, 6 Crow
Street, Dublin 2, Ireland
Sexo Explicito, (a feminist publication often concerned with
health issues), Casa da Mulher: Rua Debret, 23/13 I 6 CEP 20030,
Rio de Janeiro, R.J ., Brazil
Coletivo Feministe Sexualidade e Saude (feminist health center),
Rue Baltezar Carrasco 89, Piuheiros, Sao Paulo, S.P. , Brazil
SOS Corpo, (feminist health organization), Rue do Hospicio
859/ l 4, Recife, P.R., Brazil.
r;_~
__
Canada
Women Health Sharing, 101 Niagara St., Suite 200 A, Toronto,
Ontario, Canada
Coalition of Provincial Organizations of the Handicapped, 926294 Portage Avenue, Winnipeg, Manitoba R3C 0B9, Canada
Coalition of Provincial Organizations of the Handicapped,
Women's Caucus 456 West Broadway, Vancouver, B.C., Canada
Centre de Sante des Femmes du Quartier, 16 Est Bd., St. Joseph,
Montreal, Canada
The Immigrant Women's Centre: Mobile Health Clinic, 348 College Street, Toronto, Ontario, Canada MST IS4
Calgary Women's Health Collective, 2340 I Ave. N.W. Calgary,
AB T2N 0B6 Canada
Dis-Abled Women's Network, 122 Galt Avenue, Toronto,
Ontario, M4M 2Z3, Canada
China
Institute of Chinese Medicine, Gynecological Research Department, Zhang Jingling, Hunan Province, People's Republic of
China
Colombia
Grupo de Ajude e Inforinacion, (AIDS Information), c/o Manuel
Antonio Velanda Move, Apdo. Aereo 25770, Bogota I, Colombia
Costa Rica
Centro Feminista de Informacion y Accion, Apdo. 5355 San Jose
I 000, Costa Rica
30
Connexions 25 Winter 1987
I
J;
1£·
-'
i
Marie Falksten
© ,
Vrouwengezondheidscentrum Katelijne (women's health center),
Walstraat 5, 4531 ED Terneuzen, Netherlands
Platform Vrouwen en AIDS (women's AIDS information centre),
Maliesingel 46, 3581 BM Utrecht, Netherlands
New Zealand
Hecate Women's Health Collective, P.O. Box 11-675, Wellington,
New Zealand
New Zealand Women's Health Network, C/O Sarah Calvert, P.O.
Box 2312 Tauranga, New Zealand
Nicaragua
Festasalud, Matagalpa, Nicaragua
Nigeria
Hannah Edemikpong, Women's Centre, (information on AIDS
and genital mutilation in Africa), Box 185, Eket, Cross River
State, Nigeria, W. Africa
Peru
Italy
Gruppo Feminista per la Salute Della Donna, Vicola San Francesco a Ripa 17, 00153 Rome, Italy
Japan
Soshiren, (Committee Against Revision of the Eugenic Protection
for Reproductive Freedom, C/O JOKI, Nakazawa Bldg. 3F, 23
Arakicho, Shinjuku, Tokyo, Japan
Women's Health Action Network of Japan, C/O Japanese
Women's Council, Products Bldg., 1-33-3 Hongo, Bunkyo-ku,
Tokyo, Japan
Sapporo Group to Stop the Retrogressive Revision of the Eugenic
Protection Law, C/O Hirahira, 2F, Nishi 5-chome, Kita 18-Jo,
Kita-Ku, Sapporo City, Japan
Women's Health Center, 2-6-2 Tamatsukuri, Higashi-Ku, Osaka,
Japan
Feminist Therapy, 93-3-24 Okanouemachi, Toyonaka City,
Osaka Prefecture, Japan
Women's Body's Network "Maimai," C/O Hayakawa, 1-44
Yasakacho, Nishi-Ku, Nagoya City, Japan
Feminist Therapy, "Nakama," Rm. 302 Kihara Bldg., 17
Saneicho, Shinjuku-ku, Tokyo, Japan
Asian Women's Association,
14-10-211 Sakuragaokacho,
Shibuya-ku, Tokyo, Japan
Kenya
National Council of Women, P.O. Box 43741, Nairobi, Kenya
Breast Feeding Information Group, P.O. Box 59436 Nairobi,
Kenya
Centro de Documentacion Sohre la Mujer, Av. Arenales 2626,
Lima 14, Peru
Puerto Rico
Taller Salud, Apartado 2172, Hato Rey Station, Hato Rey,
Puerto Rico, 92172
Philippines
Gabriela, Room 221, PCI Bank Bldg., Greenhills Commercial
Center, San Juan, Metro Manila, Philippines
South Africa
Critical Health,
Central
Printing
Unit/University
of
Witwatersrand, I Jan Smuts Avenue, Johannesburg, South Africa
South Pacific
Maternal and Child Health Department, Central Administration,
P.O. Box 149, Niue Island, South Pacific
Switzerland
World Council of Churches, Elizabeth Ferris, Refugee Service,
P.O. Box 66, 150 Route De Ferney 1211 Geneva 20, Switzerland
AIDS-Hilfe Schweiz, Postfach 1054, CH-8039, Zurich, Switzerland
Dispensaire des Femmes, 4 rue du Mole, 120 I Geneva, Switzerland
Fraungesundheitszentrum, Sulgeneckstralle 60, 3000 Bern,
Switzerland
Frauenambulatorium, Mattengasse 27, 8005 Zurich, Switzerland
Thailand
Women's Information Centre, I I 3/9 Charasanitwong Road 46,
Bangkok I 0700, Thailand
Malaysia
Health Action International, P.O. Box 1045, 10830 Penang,
Malaysia
Consumer's Association of Penang, (publishes information on
women's health issues), 87 Cantonment Road, 10250 Pulau,
Penang, Malaysia
Mauritius
Muvman Liberasyon Fam, 5 Rue Street, Therese, Curepipe,
Mauritius
Mexico
IXQUIC, (published a pamphlet on women and health in Guatemala, May 1987), Apartado Postal 27-008, C.P. 06760 Mexico,
D.F., Mexico
The Netherlands
Women's Global Network on Reproductive Rights, P.O. Box 4098,
Minahassastraat I, 1009 AB Amsterdam, Netherlands
Vrouwengezondheidscentrum Utrecht (women's health center),
Maliesingel 46, 3581 BM Utrecht, Netherlands
Vrouwengezondheidscentrum Amsterdam (women's
health
center), Obiplein 4, 1094 RB Amsterdam, Netherlands
Connexions 25 Winter 1987
31
United Kingdom
Women's Health Information Centre, 52-54 Featherstone St.,
London, ECIY 8RT, United Kingdom
The New Internationalist, (an English progressive monthly which
often includes articles on women's international health issues},
120-126 Lavender Avenue, Mitcham, Surrey CR4 3HP, United
Kingdom
International Contraception, Abortion, and Sterilization Campaign, 374 Grays Inn Road, London WCI, United Kingdom
United States
National Women's Health Network, 224 7th Street S.E., Washington, D.C. 20003
Women's Occupational Health Resource Center, Columbia
University, School of Public Health, 600 W. 168th Street, New
York, NY 10032
Feminist International Network of Resistance to Reproductive and
Genetic Engineering, P.O. Box 441216, West Somerville, Mass.
02144
Reproductive and Genetic Engineering: Journal of International
Feminist Analysis, Phyllis Hall, Vice President, Pergamon Press,
Maxwell House, Fairview Park, Elmsford, NY 10523
World Health Organization/Pan-American Health Organization,
525 23rd Street, N.W., Washington, D.C. 20037
Boston Women's Health Book Collective, Box 192, West Somerville, MA 02144
International Drinking Water Supply and Sanitation Decade,
Hilda Rwabazaire Paqui, United Nations Development Programme, Room DCl-1902, One UN Plaza, New York, NY 10017
Uruguay
Colectivo Maria Abella, Ma. Stagnaro de Munar 105, Barrio
Ciccsa, Paso Carrasco, Canelones Uruguay
West Germany
Pro Familia, a health counseling centre, Deutsche Gesellschaft fur
Sexualberatung u. Familienplanung, e.V. Beratungsstelle Schluterstr. 14, 2000 Hamburg 13 West Germany
Berliner AIDS-HILFE, (AIDS Information Center), Meinekestr.
12, 1000 Berlin (West) 15
Clio, Eine Periodische Zeitschrift zur Selbsthilfe, a feminist selfhelp magazine, Feministisches Frauen Gesundheitszentrum, e.V.,
Leignitzer Str. 5, I Berlin 36 (West)
Yugoslavia
Women, Society and Health Group, Student Cultural Centre, M.
Tita 58, I 1000 Beograd, Yugoslavia
Zambia
African National Congress, Women's Section P.O. Box 31791
Lusaka, Zambia
Zimbabwe
Women's Action Group, (Publishes information on women's
health issues}, Box 135 Harare, Zimbabwe
****************************************
"ba.J.man
rower ""'/
ll 111C(\!,llZil1C' of
feminism
spiritulllity
po/;th.,
An inspiring international quarterly publication
consisting of 96 pages of the highest quality women's
literary and artistic works. Lich issue explores a theme
central to an emerging planetary woman's consciousness in
a form,lt of interviews, articles, fiction, poetry, photograph y,
art, and profiles of womrn of power. Subscriptions S22. Single
issue $6 plus $1 postage.
"] 11 these times of
,\!,relit socilll chllll,\!,C',
if WC' l/TC' to
survive its ll species,
it is JJC'CC'SSllry
for women to
come into power
uncl for
feminist principles
to rebuild
the fournlntions
of world cultures. "
-woman of power
"Statement of Philosophy"
p.o. box 827, cambridge, ma., 02238
32
Connexions 25 Winter 1987
Classified Connexions
Classified Connexions!
Connexions classifieds reach over 15,000
readers for only 30 cents per word! All
ads must be prepaid. We reserve the right
to reject any ad and we cannot guarantee
placement of ad in any specific issue.
Deadlines are the first of February, May,
August and November.
Personals
Looking for a penpal? Selling a poster?
Organizing a conference? Then your
classified
belongs
here!
Connexions
classifieds reach over 15,000 women for
only 30 cents a word . Write Connexions,
4228 Telegraph Ave ., Oakland, CA 94609
for more information or send in your ad
with payment. Display ad rates also available.
Publications
Believe in Yourself Memo Pads boost
egos, give confidence. Try them . Send
$3.75 for 1, $17.50 for 5 to: Sol, Inc. (Attn :
Connie), Box 2111 , Hyatts, MD 20784.
Retailers query.
Lesbian of Color, 30, seeks to connect
with others age 25-35, who share interest
in art, farming , true appreciation for any
peoples of color; their culture respected.
Please write Marie Douglas, 200 Vassar
Drive , S.E., Albuquerque , NM 87106, USA.
Penpals
Instruction
Call for international penpals! Wishing to
exchange letters with other women. Let's
share our experiences. Sherry Hudson ,
3060 Marshall Avenue, #314, Cincinnati ,
OH 45220.
Goddesses, goats, and green witches
learn herbal medicine and spirit healing at
the Wise Woman Center with Seneca
leader Twylah Nitsch , shaman-singer Lisa
Thiel , herbalist Susun Weed , and others.
Free brochure of workshops, retreats, and
apprenticeships .
PO
Box
64CX,
Woodstock, NY 12498.
Lesbian Woman, 25 years old , seeking lesbian support. Contact: Ebere Chukwu, c/o
Dopa
Fashion,
4
Kenneth
Road ,
Awkunanaw, Enugu , Anambia
State,
Nigeria.
Travel
VISIT NICARAGUA: Intensive Spanish
courses, family living and community work
in Esteli . Scholarships available. Apply now
for 1988 sessions. NICA, PO Box 1409-CX,
Cambridge, MA 02238. 617-497-7142.
****************************************
Subscribe to Connexions
Order two issues and
get the third issue free!
Back issues: $3.00 + .75 postage per issue
□ One year, $12
Libraries and Institutions, $24
Canada and Mexico, US$ l 4
Overseas Airmail, US$20; Surface US$ l 4
□ Sustaining subscription, $25
(Donations are tax-deductible)
Make US checks (or international money
orders and travelers' checks) payable to
Peoples Translation Service and send to:
Connexions
4228 Telegraph Avenue
Oakland, California 94609
(415) 654-6725
Is this a gift?
From
Name
Address
City, State, Zip
Send me:
□ #24 Visual Arts
□ #23 Crisis and Transition
□ #22 Facets of Racism
□ #21 Education
□ #20 Marriage
□ #19 Women's Movements
□ #17/18 Forum '85/Nairobi
($6/double issue)
D #16 Media
□ # 15 Changing Technology
□ #14 Women Inside & Out
□ #13 Women's Words
□ # 12 Prostitution
□ #11 Women & Militarism (photocopy)
□ # l O Global Lesbianism II
□ # 9 Outrageous Women
□ # 8 Culture Clash
□ # 7 Young and Old Women
□ # 6 Environment-From the Ground Up
□ # 5 Women in Eastern Europe
□ # 4 Creativity (photocopy)
□ # 3 Global Lesbianism I (photocopy)
□ # 2 In Search of Work and Refuge:
Migrant and Refugee Women (photocopy)
□ # l Women Organizing Against Violence
(photocopy)
(Issues 1, 2, 3, 4, and 11 are only available
as photocopies)
Peoples Translation Service
Connexions
4228 Telegraph Avenue
Oakland, CA 94609
(415) 654-6725
$3.00
Non-Profit Organizatior
U.S. Postage Paid
Berkeley, CA
Permit No. 148
-
An_ International Women 's Quarterly
The Politics or
HEALTH
1 Introduction
2 India: Eliminate Inequality, Not Women
The abuse of amniocentesis may lead to female extermination.
4 Britain:
Robbed of Colour
Due to vitiligo, a Black woman is losing her color.
6 Senegal: Change the Mentality, Not the Skin Color
Black women are pressured to lighten their skin with dangerous compounds.
7 Britain: Fat Women Fight Back
Fat women fight societal standards of health and beauty.
8 Canada: Screaming in the Wind
A woman reports on her many years of experience in mental institutions.
10 West Germany: Sterile Without Consent
Disabled women are being involuntarily sterilized.
12 Update: Restricted "Choice"
Abortion rights updates from Ireland, Israel, India, Hong Kong, Mauritius and Japan.
15 Costa Rica: The International Meeting on Women and Health
Women exchange resources and information.
16 Nigeria: AIDS Linked to Genital Mutilation?
Hannah Edemikpong discusses a possible correlation between genital mutilation and AIDS in Africa.
18 India: Cooking Inside
The effect of wood smoke on the health of women.
20 Kenya: Water: An Obstacle for African Women
Women's water projects help to provide better quality drinking water and sanitation.
23 Canada: Woman and Substance Abuse
Women work together to fight substance abuse.
24 Collectives:
Together We Are Strong
Women organize for better health in Switzerland, Berlin, Bangladesh, Mauritius, and Nicaragua.
26 Shorts:
Health shorts from Malaysia, Canada, Switzerland and New Zealand.
29 Letters
30 Health Resources for
Women
Office Staff
Constantina Bertone, Linda Fogel, Shoshana Friedkin,
Pally Ruppel!, Anne-Marie Schmoltner, Donna Scism,
Patricia Sieber, Iris Wesselmann.
For This Issue
Editorial
Constantina Bertone (co-coordinator) , Amy Christiansen , Karen Hayashi , Leslie Jones, Viki Radden , AnneMarie Schmoltner, Donna Scism (co-coordinator),
Patricia Sieber, Janis Steele, Iris Wesselmann.
Production
Constantina Bertone (coordinator, typeselling), Dee
Elling (cover), Linda Harrold (proofreading), Leslie
Jones, Leslie Katz, Ellen Owens, Pally Ruppelt (typesetting), Donna Scism (typese11ing), Janis Steele, Iris
Wesselmann
Translation
Viki Radden (French), Anne-Marie Schmoltner (German), Donna Scism (Spanish), Patricia Sieber (German ,
French)
Special Thanks To:
Mark Manzione, Ines Rieder
Statement
Connexions is the collective product of feminists of
diverse nationalities and political perspectives committed to contributing to an international women's movement.
We want to go beyond merely providing facts
and information, and hope that by passing on-as
directly as possible-women's writing generally unavailable in the US, we will be helping women here to
understand and connect with the experiences and
viewpoints of women in other parts of the world. We
also want to contribute to the growth of a worldwide
network connecting women working on similar projects
by researching, establishing contacts and exchanging
information with other women 's organizations.
To a large extent, the economic and political
conditions under which we live determine the issues to
which we give priority. Women do not live in a
vacuum, but in what is still largely a man's world. It is
essential for us to understand the working of that world
if we are to understand each other. We hope that Connexions will be one step toward building an international women 's movement.
Connexions is a quarterl y and each issue focuses on a
specific theme. Connexions is published by People's Translation
Service. 4228 Telegraph A venue, Oakland. CA 94609. Subscription rates are $ I 2 per year: Canada and Mexico US$ I 4:
Overseas-US$ I 4 surface. US$20 airmail. An annual institu•
tional subscription is $24. Please send international money orders in US$ or international travelers' checks in US $.
Articles and photographs from Connexions may be
reprinted free of charge by non-profit publications without per~
mission except where accompanied by cop yright. (Others please
inquire for reprinting rights.) Please credit Connex ions. including
our subscription rates and address whene ver reprinting our
material. and please send us a tearsheet. Connexions is indexed
in th e Aliernati,·e Press Index, P.O. Box 7229. Baltimore. MD
2 1218.
ISSN 0886· 7062 .
The Politics
of HEALTH
SAMPL~ COPY
Who is concerned with women's health? Those who have power over
women's health issues often show little concern. Because females are in
many societies less valued than males, a plethora of health problems
arise. One of the most blatant examples is the abuse of amniocentesis
in India. A recent Indian report states that 7,999 of 8,000 fetuses
aborted after amniocentesis were female. Another example is the forced
sterilization of mentally disabled women in West Germany. Such practices as these shatter the common myth of the neutrality of science and
technology.
Pressure to conform to certain standards of beauty-beauty being
one of the chief societal measures of a woman's worth-can incite
women to do great harm to their health. Black women in Senegal, living
under the colonial legacy that light-skinned women are the most desirable, use dangerous compounds to depigment their skin. Fat women are
urged to become thin by surgical and other means that can damage
them permanently. Women working to counter this destructive situation
urge that it is society that needs changing, not women's bodies.
Women's health is often endangered by something more fundamental than the demands of beauty. Work-both the quantity and the conditions under which it is done-can wreak havoc on a woman's well-being.
For example, in India, women do most of the cooking. A lot of cooking in
rural areas is done over a wood or dung fire, often in unventilated structures. The woman cook continually breathes smoke, which contains large
quantities of pollutants. Respiratory diseases are a leading cause of
death among girls and women over the age of five in India; smoke inhalation is thought to be a major factor.
In rural Kenya, women must walk many miles each day to collect
water. During the dry season, collecting water can be so time consuming
that the woman has little time or energy left for her other duties.
Refugee women, who are already under tremendous strain from
being uprooted, often face special health problems as pregnancy and
breast-feeding exacerbate their malnourished state. Also, because
refugee women are often responsible for collecting fuel and water and
for taking care of the children, they are the last to receive health carethey don't have the time to go to a health clinic.
Women's health collectives and self-help projects are helping
women gain control over their own health and bodies. They emphasize
preventive medicine, provide alternative treatments such as acupuncture
and homeopathy, make health care affordable and available, and provide
information on contraception and abortion. These groups are committed
to creating an accessible network of health resources for women.
Valuing ourselves and our health is an important part of change and
of healing. But women also need to regain the power to make decisions
regarding individual and collective women's health issues. In societies
"where looks and sexuality are used to control women, we need to
question all physical and behavioral norms imposed on us.'' Marching
against restrictions on reproductive rights, denouncing societal standards
of beauty and health, disseminating improved wood burning stoves in
India-all are examples of efforts to put women's health and control over
our bodies back into the hands of women. D
Connexions 25 Winter 1987
1
Eliminate Inequality,
(By Vibhuti Patel, Women's Centre, Bombay, India.)
Amniocentesis is a scientific technique that was intended to be used in
detecting genetic abnormalities of a foetus.
In India, it is currently being widely used
as a means for sex-determination. By comparison to other countries, amniocentesis is
quite inexpensive in India. Hence, not only
upper class women , but even working class
women have access to the test. A recent
survey of the slums in Bombay revealed
that when women found out their foetus
was female, many chose to abort. Many
argued that it was better to spend a bit of
money now for an abortion than to have to
pay a fortune for a girl's future marriage.
The controversy began a few years
ago when the results of several investigative reports were published in popular
Indian magazines and journals. Many of
the results were horrifying. Of 8,000 abortions following amniocentesis, 7,999 were
found to involve female foetuses. In addition, between the years 1978 and 1983, it
is estimated that 78,000 female foetuses
were aborted after sex-determination tests
in India.
The government and private practitioners involved in this lucrative trade justify the sex-determination test as a measure
for population control. Women have
always been the ones burdened with the
effects of family planning policies. Harmful
effects of pregnancy tests, contraceptive
pills, anti'-pregnancy injections, and unhygienic camps for mass sterilisation of
women are just a few of the drawbacks
often overlooked by enthusiasts of family
planning policy.
India has a history of killing female
children (dudhapiti) by putting opium on
the mother's nipple, by putting the afterbirth over the child's face , and by illtreating its daughters. Even today, female
members of the family get inferior treatment as far as food , medication, and education is concerned. When a girl grows up,
she is further harassed about her dowry.
Many social scientists ask whether or not it
is better to die rather than be ill-treated.
In the words of Dharam Kumar, "Does the
birth of...millions of unwanted girls
improve the status of women?" To think
that it is better to kill a female child or
foetus than to have a child whose sex is not
highly valued in society is fatalistic. Next,
2
Connexions 25 Winter 1987
people will rationalize that it is better to
kill the poor rather than let them suffer
poverty and deprivation! How horrifying!
But what can be the long-term implications if such trends continue? Won't it
further aggravate the already disturbed
sex-ratio? There was a large and steady
decline in the female/male ratio in India
between 1901 and 1971. Between 1971 and
1981, there was a marginal increase in the
ratio, although women are still outnum- •
bered by men. [India is one of the few
countries in the world where the femaleto-male ratio is declining.) Economists
often say that if the supply of women is
reduced, women's status will be enhanced.
According to this logic, women won't be
burnt alive because of insufficient dowrybecause they won't be an easily replaceable
commodity. But the economists forget the
socio-cultural milieu in which women have
to live. A society that treats women as
mere sex objects will not treat women in a
more humane way just because they are in
scarce supply. On the contrary, in many
local communities, there is a negative
correlation between the female/male sex
ratio and the incidence of rape, abduction,
India
Not Women
"Don't kill your daughter after sex-determination tests."
"Stop sex-determination tests offetus in the womb. "
and forced polyandry.
Another argument in favor of sexdetermination tests is one which touts the
myth of the ideal "balanced family." It is
argued that women who have one or more
daughters should be allowed to abort their
daughters and try again to produce a son.
This concept of "balanced family" is
extremely sexist and very frightening.
Would a couple with one or more sons
undergo amniocentesis to get rid of a male
foetus, just so that they could have a
daughter in order to balance their family?
No, never!
Time and again it is stated that
women themselves enthusiastically go for
the test out of their own free will. "It is a
question of a woman's choice." But, are
these choices made in a social vacuum?
Indian women are socially conditioned to
believe that unless they produce one or
more male children, they have no social
worth. They are harassed, taunted, and
even deserted by their husbands and inlaws if they fail to produce a male child.
Thus, their 'choices' are limited by their
fear of ridicule by society. It is true that
feminists all over the world have
demanded the right of women to control
their own bodies and choose whether or
not to have children. They have also fought
for free, legal and safe abortions. But these
issues should be viewed in a different context in Third World societies because
imperialism and racism are often major
forces working to control coloured populations. Population control advocates often
endorse women's rights and then divert
attention from the real causes of the population problem: the lack of food, economic
security, clean drinking water and safe clinical facilities. These factors have created a
situation where women must have between
two and six children in order to have at
least one surviving male child. This is the
root of the population problem.
Abuse of amniocentesis shatters the
myth of the neutrality of science and technology. Just as the invention of atomic
energy was used to destroy Hiroshima and
Nagasaki, so could sex-determination tests
be used for female extermination.
We at the Women's Centre are
undertaking educational campaigns to help
combat this problem. Most women's
groups feel that amniocentesis should be
permitted only under strict governmental
control and only for the detection of
genetic abnormalities. To consistently campaign against the notorious activities of
money-minded doctors and the antipathy
of the government, the Forum Against
Sex-Determination and Sex Preselection
was formed in Bombay in 1986. As a
result, the issue has gained nationwide publicity and the government has begun to
respond favourably. In March 1987, a committee was appointed to study the proposal
to stop the misuse of sex-determination
tests. We are hopeful that the government
will help to prevent the situation from
leading to further female extermination. D
Contact:
• Women's Centre, 104B Sunrise Apt.,
Above Canary Bank, Nehru Road, Vakola,
Santacruz (East}, Bombay 400 055, India.
Further Reading:
• "Action Against Sex-Determination and
Sex Preselection," Womennews, newsletter
of the women's centre, Bombay, India,
August 1987.
Connexions 25 Winter 1987
3
Britain
Robbed of Colour
(From "Robbed of Colour," by Sarojini
Ariyanayagam in Spare Rib, British feminist monthly, #173 December 1986.)
As a Black person, the last thing I
would want is to turn white. Yet this is
precisely what is happening to me. I am a
33-year-old Tamil woman from Sri Lanka.
I am very dark-skinned. At the age of 17, I
developed vitiligo, a condition in which
cells in the skin stop producing pigment.
An estimated 50 million people throughout
the world have this condition, yet most
people have never heard of it. This is probably related to the fact that, although
vitiligo can strike anyone regardless of
colour, it is Black people in particular who
bear the brunt of its traumatic psychological effects. For sixteen years, I have been
waging a battle against a process which is
gradually robbing me of my colour and my
identity.
When the first white patch appeared
above my eye, I assumed it could be
treated by a doctor. But the dermatologist
diagnosed it as vitiligo, informed me there
was no cure, and then dismissed it as a
condition I'd "have to learn to live with." I
was heart-broken. Every new spot that
appeared on my neck, face and arms just
increased my anxiety. By 1985, I had lost
80 percent of my pigment. Can you imagine the trauma of this happening to you?
Imagine how a white person would feel if
she suffered from a hormonal condition
and her skin gradually turned black?
Perhaps at this point, I should tell
you about the nature of vitiligo. It can
affect anyone, at any age. It may be triggered off by emotional stress or physical
injury. According to one theory, the body
develops antibodies to melanin, the pigment in skin. Common sites of vitiligo are
the face, genital areas, hands and hair. It is
not infectious and often appears symmetrically. It is generally a progressive condition, although in some cases patches
remain the same for years or spontaneously
re-pigment. Vitiligo affects 1-2% of any
population. Dark-skinned people in the
Third World suffer the most from the
consequences of this condition since the
loss of pigment makes one more susceptible to skin cancer. On the whole, however,
still little is known about vitiligo. A parallel can be drawn between vitiligo and sickle
4
Connexions 25 Winter 1987
cell anaemia: as they both particularly
affect Black people, the resources for
research into those conditions is not
readily available.
As with other skin conditions, like
eczema and psoriasis, one of the main conventional treatments for vitiligo is steroid
ointments. However, these should only be
used for short periods of time as they thin
the skin. The alternative is psoralen tablets
combined with ultraviolet light (PUVA).
This drug makes you very sensitive to the
ultraviolet light for a number of hours and
can have unpleasant side-effects. Furthermore, prolonged exposure to UV light can
cause skin cancer. PUVA is also used for
psoriasis. Both these treatments have a
very limited success rate and in some cases
can aggravate the condition. In Africa and
Asia, herbal treatments are commonly used
with some success.
In my case, my mother couldn't handle what was happening to my skin; she
confused vitiligo with leprosy; so I had to
cope with an incurable and rapidly
disfiguring condition on my own. At that
point, I went into a depression that lasted
until my late twenties. I would always wear
long-sleeved clothes, and try to cover up
my neck. When I saw myself in photographs, I realised that I was "deforming"
my shoulder in order to hide my neck. I
felt myself changing into a shy, overly sensitive and defensive person. Looking back,
I wish someone had encouraged me to get
the emotional support and help I needed.
Having tried all the standard treatments various doctors had to offer, I
started the rounds of "alternative therapies." I spent a lot of money paying for
treatments. After eighteen months, I realised that I wasn't getting anywhere.
Recently, however, I've gained some hope.
I just returned from Cuba where I was
treated by Dr. Cao-he believes that
vitiligo is a psychosomatic disorder; however, the physiological consequences are
not fully understood. His treatment is
based on an extract from the placenta
called melagenina. The lotion is rubbed
into the skin twice a day, and applied
under infra-red lights once a day for 15
minutes. The protein helps speed up the
oxidation process in the chemical pathway
of melanin production, thus stimulating
melanin synthesis and multiplication of
melanocytes.
After three months of treatment, my
condition improved remarkably. It is hard
to believe that only a year ago I had almost
given up hope. The effort involved in
"making up" for the outside world and trying to look "normal," had exhausted me. It
was a lonely struggle, and I was too
ashamed to talk about it. I helped to organize the Vitiligo Group because I needed to
talk with people whose condition was similar to my own. For most of us in the group,
it was the first time we'd met anyone else
with vitiligo. We found we were all saying
the same things and facing similar frustrations. The silence and pretence was over.
Being together, we could take some positive action, and begin research into all
aspects of the condition. Meeting in this
group has changed our lives.
We are now a national charity of 400
members, including a medical and research
team. At least 75% of our members are
women even though vitiligo affects both
sexes equally. The conditioning we've
received as women about the importance
of our appearance makes us react to
vitiligo differently than men. Everywhere
Ingrid Pollard/Spare Rib
we look, we are presented with images of
the model woman, no blemishes, perfect
skin, beautiful looks, and almost habitually
we adapt to the social norm. Women in the
group take "naturally" to camouflaging
their "disfigurement," dying their hair.
Women with vitiligo often feel very
desperate about sexual rejection. A couple
of women even tried having their white
patches painfully tattooed.
While I was in Havana for three
months, I met many other vitiligo sufferers
from Venezuela, Mexico and Brazil. Some
had already started re-pigmenting which
was very encouraging to me. Dr. Cao
advised me to give up camouflage make-up
in order to keep my skin clean for treatment. I hadn't done that for 15 years! It
was wonderful to be accepted as I am.
Unlike in this country, people in Cuba
didn't stare at me because of my
disfigurement. In that society, you're not a
freak for looking different.
You 're
accepted for who you are. I was very lucky
to receive the treatment free as a reward
for my work with the Vitiligo Group.
I have a tremendous amount of hope
and believe that there is a potential in
melagenina for curing vitiligo. With further
research and expertise, its effectiveness
could be increased and it could be made to
work faster. A dermatologist from England
has decided to visit Dr. Cao in Cuba to
study the progress of his patients and his
methods of research. Hopefully, it won't be
long before British vitiligo sufferers will
have access to the sort of treatment available in Cuba. □
Further Reading:
• Vitiligo and Other Hypomelanoses of the
Hair and Skin, By Jean-Paul Ortonne, Plenum Medical Book Co., New York, 1983.
Connexions 25 Winter 1987
5
Change the Mentality,
Not the Skin Color
(Translated from Fippu, Senegalese feminist trimestrial, no. I July 1987.)
In the 1970s, skin-lightening in Senegal was the cause of much debate, and a
source of embarrassment for many. However, now that "Black is Beautiful" has
long since ceased to be a rallying cry for
the world's blacks, skin-lightening is once
again in fashion. Beauty and medical
experts alike tell of the wonders of skin
lightening, promising a better love life and
improved self-esteem. This advice is given
much to the dismay of those in the
women's and social service communities,
who are concerned that these experts never
mention the dark scars and blemishes that
mar the skin after these often toxic products are applied. They speak only of the
glamor of having clear, even-toned skin,
not of the mercury poisoning, lupus and
blood disease. These are only some of the
many ailments that often afflict those who
choose to chemically lighten the color of
their skin.
Skin is composed of two layers: the
dermis and the epidermis. The epidermis,
which contains an immense network of
nerve endings, is the outer layer which protects the sensitive dermis underneath from
extremes of temperature and from the
sun's harmful rays. With only basic care,
the skin can retain its protective and elastic
qualities for years.
The products used for skin lightening, however, break down the skin's natural
protective barriers. Skin lighteners contain
mercury salts, peroxides, and other
ingredients which are unspecified. Some
methods involve cortisone injections or
topical applications. All of the compounds
are dangerous, particularly those whose
chemical compounds are not completely
known. Treatment of the disorders resulting from the use of these compounds must
be given under strict medical guidelines,
which is often painful and costly. This is
because the products used for treatment in
Senegal are either in pommade form
(cream), or in solid or liquid soaps, where
the methods of application and use can
vary greatly from one woman to the next.
Skin lightening is usually done in
three steps. First, the product (or products) must be applied and allowed to
remain on the skin all ·night long to facilitate the depigmentation process. The epidermis must be modified in order for
depigmentation to begin. Next, on the following day, an even stronger combination
of products is applied. The length of time
6
Connexions 25 Winter 1987
the products remain on the skin depends
upon the desired effect . The final step
involves the maintenance of the depigmentation process. Creams are not usually
used at this stage, since maintenance is
achieved by the use of various soaps and
skin cleansing products.
Accidents which result from the use
of these products abound, in spite of the
fact that beauty experts insist that skinlightening is just another "beauty treatment." In Dakar, Senegal's capital, these
accidents account for I% to 2% of all dermatological consultations. They include
toxic reactions to the products, damage to
blood vessels and the entire circulatory system, with injuries to one or more major
organs such as the heart, liver or kidneys,
and to diseases of the veins from the prolonged use of mercury salts, which can
bring about many types of neurological
disorders. Not to mention what can happen during treatment of these maladies:
there is always the risk of serious postoperative infection.
Senegal
"... women with clear, light skin have more
sex-appeal than others: we notice them
more! In fact, I began the skin-lightening
process because I know some women who,
having naturally dark skin, weren't beautiful, but who became very seductive from
using the products."
Many Senegalese women like Khady
feel pressured to lighten their skin so they
will be more attractive to their mates. A
large percentage of women who use the
products, in fact, are women whose husbands have brought the skin-lightening
techniques home for them to use. Women
in Senegal are still valued more for their
ability to attract men and bear children
than for their other qualities.
Men such as Lamine, age 40, make
dark-skinned women feel inferior and unattractive. Lamine, an intellectual, has a
dark-skinned wife, but he doesn't miss any
opportunity to tell either his wife or his
friends that he has a firm intention of marrying a second time, and this time, a lightskinned one!
"J prefer light-skinned women, and that's
that!" he says.
While some may prefer light skin
and extol the virtues of skin-lightening products, the women's community will continue to speak out against the practice.
They say it is threatening to the Black race
itself and an embarrassment to the country
whose former president, Leopold Senghor,
was one of the founders of the Negritude
[Blackness] movement. Skin lightening, as
Marietou, age 45 , says:
Yet skin-lightening continues to be
widely practiced in Senegal. Why? Some
apparently feel that beauty is worth achieving at any cost, and to them, ebony-colored
skin is not beautiful. Even though some
men are now using the skin-lightening products, the majority of the users are women,
from all age groups and social backgrounds.
Khady, a 22-year-old Senegalese
woman, tells us why she took the risk and
lightened her skin:
" ... is sad for a country that has always been
on the cutting edge of the war for the revitilization of the black race... and the degree of
skin lightening coincides with the degree of
alienation: the more light-skinned you are,
the more you are considered as an object to
covet! We must enlighten the women as well
as the men and reverse the canons of
beauty... Me, I am black and fit quite well in
my skin ... "
Marietou's advice to the women of
Senegal? "Changer de mentalite et non pas
de teint" (Change the mentality, not the
skin color). □
Contact:
• Fippu, a Senegalese feminist trimestrial,
B.P. 4163, Dakar, Senegal.
Fat Women Fight Back
Britain
(From SpareRib, British feminist monthly,
No. 182, September 1987.)
We are fat women who want to challenge the myths about fat. We want to
stress that fat is not always a question of
personal choice and control; neither is it a
visible sign of failure. The issue for us is
not why we are fat, but why we are treated
badly because of being fat.
Contemporary Western culture promotes an increasingly thin ideal; we have
found no positive images of fat women in
the mainstream media. Quite the contrary,
women's magazines and the media in general just focus on how to get rid of fat. In
a society where looks and sexuality are
used to control women, we need to question all physical norms imposed on us. We
should work towards self-acceptance and
self-love irrespective of the size of our
bodies.
A thin woman may suffer because
she cannot attain an impossibly thin ideal.
Fat women, however, are harassed and
discriminated against regardless of how
they themselves feel about their bodies:
society at large thinks that there is something fundamentally wrong with fat
women.
In Britain, fat women are continually
pressured to lose weight. Moreover, fat
women experience direct and indirect
discrimination in job selection and harassment at work. Fear of ridicule often
prevents us from taking part in sports and
leisure activities such as dancing and swimming. Public transport and the design of
public spaces often excludes fat people;
seats are too small and there is very little
space in pubs, restaurants, cinemas. In
school, fat children can be ridiculed by
peers and stereotyped by teachers. The
majority of clothes shops sell nothing we
can wear. The media degrade us, defining
us as a problem which needs to be eradicated; we are stereotyped as lazy, pathetic,
out of control, stupid, ugly, jolly, maternal,
asexual or sexually ravenous.
On top of all this, fat women are
often thought of as being greedy. Because
body size is often mistakenly linked with
food consumption, fat is defined as an eating disorder. While some fat people, like
some thin people, are or have been compulsive eaters, many do not have problems
with food. In fact, most fat people know
that we do not necessarily eat more than
most thin people. Yet both the diet and
medical industries promote the idea that
no matter how little a fat person eats, it is
too much if she remains fat. We have to
examine whose interests are really being
served by this idea. The market is flooded
with diet fads, pills and foods. The diet
industry is multinational and extremely
profitable. Ironically, the highly profitable
Weightwatchers is owned by a food company. Furthermore, an increasing number
of researchers from the Medical Research
Council and the Department of Health
Investigating Committee have come to the
conclusion that diet foods can be not only
expensive and ineffective, but outright
dangerous.
Good health is usually cited as the
most important reason for losing weight.
Fat women are perceived as medical prob-
!ems; regardless of whether we have a
sprained thumb or a common cold, our ailments are automatically attributed to our
fat. We are often denied proper treatment
until we lose weight; then we are mutilated
in the interests of "good health." We know
that some fat women have had their jaws
wired, many more · have used and become
addicted to diet pills, and some have even
undergone plastic surgery. Such procedures
often turn healthy fat people into ill thin
people. Side-effects include malnutrition,
diarrhea, vomiting, hernias, stomach perforation and spleen injury. It is an indication of the suffering and humiliation fat
people experience in their lives that many
are prepared to undergo these operations.
So it is not necessarily fat, but fat
oppression that can damage our health. We
are physically and emotionally hurt by
external and internalised oppression, and
then we are blamed if this results in ill
health-as if health or size were simply a
question of individual choice and control
and were divorced from social and political
issues.
If you have dieted a lot and always
end up getting fatter, you learn that you
don't have a choice about your size: either
you can blame and hate yourself or you
can choose to challenge those that oppress
you and refuse to be victimised. It is a political act for a fat woman to get angry
about the way she is oppressed and to stop
believing she deserves such pain and degradation.
Most of us might already be challenging fat oppression in our lives, but it is
important that we organise collectively to
ensure that our views are made part of a
wider political agenda. We can attempt to
build a network of support groups and
activities. We can set up local swimming
and exercise classes for those fat women
who choose and are able to participate in
such activities. We can challenge the
clothes industry, which fails to meet our
needs (even though about half the women
in this country take a size 16 or over) and
encourage the setting up of co-ops that
make clothes fat women want to wear. We
need to challenge the medical profession
and demand our right to adequate health
care. We can campaign against oppressive
industries which exploit, abuse and humiliate fat women. We can challenge negative
representation of us in both the mainstream and alternative media.
We must make ourselves and other
people aware of the fact that being fat and
beautiful are not mutually exclusive; people
should love us for who we are and not in
spite of the fact that we are fat. To stop
punishing ourselves is just a beginning-we
still have to affirm our right to, quite
literally, take up space. We demand pleasure and fulfillment as fat women now, not
in some thin future. It is society that has to
change, not us. □
Further Reading:
• "How Society's Obsession With Thinness is Consuming Women," Herizons,
Canadian
feminist
magazine,
October/November 1986.
Connexions 25 Winter 1987
7
Screaming in the Wind
(From Makara, Canadian
three/Number one.)
women's
quarterly,
Volume
The following are excerpts from taped conversations between
Molly Dexell and MAKARA's Nora D. Randall. Molly spent
almost twenty years going in and out of mental institutions.
Q: Why do people go into mental institutions?
A: There are two reasons why people go into a mental hospital.
Either they can't function, or they do something that looks crazy
to other people. Now suppose you've got a mother of six kids
who is so depressed that she can't get up in the morning.
There's a two-year-old starving, and the mother still can't get up.
Oftentimes the mother will be institutionalized because she can't
cope with everyday life. Why couldn't the family just hire someone to help out with the kids and give the mother a chance to get
better? She could visit her shrink at the day hospital and come
home at night. It is very hard to deal with getting well and raising children simultaneously. It was hard enough for me and I
only had one child. They'd be saving money by not institutionalizing her, and they could keep the whole family together.
Q: How do you see the relationship between psychiatrists and
mental patients?
A: People who haven't been mentally ill are not totally aware of
what the whole thing is about, although some act as though they
do. Psychiatrists don't have a chance of being successful at helping mental patients until they accept the fact that only the mentally ill really know what their sickness is all about. Once they
have had one year of college psychology, many student doctors
diagnose themselves as being "schizophrenic", "catatonic", and
all that shit. I've had some of them say to me, "I'm a potential
mental patient." Well, sure, the whole world is. I say,"Do you
know what it's all about to hear a voice? Do you know what my
voice is all about?" It irks me so badly, to hear that kind of
drivel. Another thing I've learned from experience is that you
don't tell psychiatrists in the hospital about anything important.
You don't even tell them you don't like baked potatoes. You talk
about all kinds of things you think they want to hear. You have
to go to them for your medication, you see, you're tied to them;
you need the medication and you know it, and there's no way
you can get it without going to a shrink.
The job of getting well has been taken right out of your
hands-the psychiatrists handle it. It's really your problem and
you're the one who knows it. There isn't a psychiatrist who
knows more about me than I do. The only thing that's going to
save mental patients is mental patients. The psychiatrists are
there to help save themselves. But they take it out of our hands
and blow us out with shock treatments and pills and all the rest
of it. That is no way to cure mental illness. That's proven by the
return to institutions of so many mental patients-old mental
patients who have had the problem recur because it isn't properly fixed the first time: You can have a breakdown and another
breakdown and another breakdown, and eventually you yourself
must work your way out of it.
8
Connexions 25 Winter 1987
Q: Don't you think mental patients could work their problems out
sooner if the way they were treated in the hospital wasn't so
literally sickening?
A: Yeah, it's really a lousy setup. I had hope because I had a
good psychiatrist. If you've got a good psychiatrist, someone who
values intelligence, she or he is concerned about fear. Fear is the
greatest emotion that mental patients have. Anger is another
great emotion. And the anger is a result of your fear. The fear is
beyond belief... beyond the conception of the ordinary person.
Q: Do you think it is fear of the actual illness itself, or fear of how
you'll be treated because you are sick?
A: Well, both. The intense illness is frightening. But I think it's
intensified in the hospital.
Canada
Q: Knowing what you know now, if a doctor ordered shock treatments for you, would you kick up a fuss?
A: No way. If you kick up a fuss in a mental hospital, you get
locked up. I wouldn't kick up a fuss in the hospital. That's the
craziest thing I've ever heard. Why, they'd just pick you up and
carry you in, that's all. I've seen a 70-year-old woman, screaming and fighting, picked up and carried in. Once you see that
happen, people get educated. That's the biggest shock in a mental
hospital. I hesitate to compare these-it sounds a little
paranoid-but it must be the same feeling that political prisoners
had during Nazi Germany, during the extermination. People
were picked up and terrible things happened to them, while the
rest of the world was ten miles away and didn't know what was
happening.
It's the same at Riverview. Totally helpless, cut off, nobody
relating to you, nobody understanding what's happened to you,
and there's this screaming in the wind. That's a feeling you have,
and you don't ever get over it. It never leaves you. I would be
very, very slow about putting anyone in a mental hospital for the
first time. When you go, you .see things and learn things you
never forget. No matter what you do, where you go, you're
always afraid you'll be put back. Your whole life is taken totally
out of your hands and it's put in the hands of ruthless people.
When psychiatrists learn to relate to their patients, then they will
have learned a little about psychiatry.
Beyond Sound
My day is a snare
In which I am caught
Struggling.
At dawn I am revived
To continue
What has become to me
A life outside of life
Where my soul screeches
To unimagined heights
And instinct holds me back,
Puts on the brakes,
Till gathering strength
I quietly descend to the glassy surface
And I remain,
Healing myself
By the steady routine of my existence
And yet,
I am not healed,
For a word
A distant threatening sound
Q: Is there a place for mental hospitals?
A: Not called mental hospitals. There should be a place. Someplace restful, where they could have a holiday-Hawaii. D
Shoots me off again
Shattering the cobwebs
That enfold me
Encircle me
Bind me
To some hidden sorrow
That lies there in a stupor
At the back of my head.
There is no word
That accurately describes
The feeling of foreboding that I once had
That now slides past like some reptile
Nudging at the corners of my eyes.
Let me look away;
Let me see the things I love.
How wonderful!
How beautiful!
But it is still there!
When will I feel safe again?
Never?
(By Molly Dexell)
All graphics by Marie Falksten
©
Further Reading:
• Women and Therapy, a feminist quarterly, Hawthorne Press, New York.
• I'm Not Mad, I'm Angry, Dorothy Smith
and Sara Davids (eds.), Press Gang,
Vancouver, B.C., 1975.
Connexions 25 Winter 1987
9
Sterile Without Consent
(Excerpted from Connexions' interview with Theresia Degener,
December I 987.)
Theresia Degener is an active member of the West German
disabled movement. She is particularly interested in the issues surrounding the involuntary sterilization of disabled girls and women.
She has published a book about disabled women and has written
an article on this subject which was published in Emma, a West
German feminist magazine, in August 1985. Theresia is currently
a law student at the University of California, Berkeley.
In 1984, the West German media started to pay attention
to the issue of sterilization. This was partly due to the discovery
by htstorians that many of the girls in schools for the mentally
disabled had been sterilized without their consent or against their
will. After these findings were publicized, a television program
"Panorama" was devoted to this topic. On "Panorama," a
mother explained that she had had her disabled daughter sterilized at the request of her daughter's teacher. The teacher
requested sterilization because the children were going on an
overnight field trip and he did not want to be responsible in the
event that the girl engaged in sexual activity and became pregnant.
In fact, many institutions in West Germany require the
sterilization of mentally handicapped girls as a prerequisite for
admittance. The institutions don't want to deal with the possibility of a pregnant disabled woman. Parents of disabled teenagers
are often intimidated by the sexuality of their children and are
fearful of a potential pregnancy.
"Panorama" alerted the public to these issues-many
Social Democrats and much of the alternative press were
horrified at these findings. Many who protest this abuse of sterilization draw parallels between the current situation and the
forced sterilization that occurred under the Nazis. An estimated
400,000 people were sterilized against their will or without their
consent during the Nazi era. Currently, there is a heated debate
about whether or not the federal government should provide
compensation for those who underwent forced sterilization.
The present West German criminal code clearly states that
sterilization is illegal unless it is performed with the consent of
the affected and if this consent is not against ethical principles.
Sterilization against a person's will or without her consent is only
permissible if there is a present danger to the health of that person. However, some people claim that there is a gap in the law,
in that it does not say anything about those who are mentally
unable themselves to give consent. Some intermediate courts
have ruled that the consent of the disabled can be replaced by
the consent of the parent or _legal
representative in cases
where the disabled person is incapable of making her own decision. This is not legal, however, as the law does not allow for this
option. The legal system in West Germany is not a case system
like the United States where the rule of precedence must be followed. Courts in West Germany do not look to precedents set by
other courts, but rather they must find the answer in the law
itself.
Lebenshilfe, the largest organization for the parents of the
disabled, is one of the main proponents of involuntary sterilization. It was founded in the 1950s and it runs "sheltered
10
Connexions 25 Winter 1987
workshops"-a place where disabled people are employed. It
runs several other institutions and even has its own publishing
house. Lebenshilfe and many other parents not organized in
Lebenshilfe want a new law legalizing the sterilization of the
mentally disabled because they don't want their children to
become pregnant. Many of the parents feel that because they
have already exerted so much energy raising a disabled child,
they don't want the burden of raising their children's children.
They claim that sterilization is in the best interest of the kids
and that there is no place within the institutions that could
accommodate a pregnant mentally disabled woman. The common morality on this subject is that the mentally disabled db not
have a right to reproduction.
In the 1960s and 1970s, not much was known about how
many people were affected by this practice of sterilization, but
recently teachers in Hamburg have revealed that about 30% of
the girls in special schools for mentally disabled children have
been sterilized. These girls are less than 18 years old-most of
them are less than 14. It has been easy for parents to have their
kids sterilized; doctors agree readily. On the other hand, for
able-bodied women, it is very difficult to get a sterilization. If
they are under 18, it is illegal.
The federal government started an investigation to find out
how the federal states and institutions are dealing with the problem. A special board was created to work out a statute which
allows for sterilization without consent. Special education experts
say also that what has been done in the past should be made
legal.
One major concern parents and institutions have is rape.
Many mentally disabled women are raped in institutions, by relatives, and in the streets. However, there are no available statistics
on the subject. Mentally disabled women are in particular
danger because they cannot communicate the same way we communicate; they can be easy victims. Proponents of sterilization
claim that they want to prevent the repercussions of rape,
namely conception, since many of them are Catholic and cannot
agree with abortion. I think it is very cynical to deal with the
problem of rape by sterilizing disabled women.
Eugenics is another concern. There is a big discussion
about eugenic thinking and of new developments in the fields of
genetic engineering and reproductive technology. Udo Sierck,
who is disabled and has done a lot of work on this issue, has
discovered that some genetic counseling offices which are provided by the state in West Germany also provide sterilization
recommendations for other doctors. The recommendations are
most often based on social behavior: If you are in a special institution, if your father is an alcoholic, if your uncle is unemployed,
if your brother is also in a special institution, you are diagnosed
with an inherited disability, and sterilization is recommended.
The eugenic arguments used by these counseling offices are
currently a hot topic in West Germany, because they remind
people of the population control the Nazis planned. Some papers
were stolen from some of these offices and published, which was
very embarrassing for the people working there. They had
difficulties saving their jobs and justifying genetic counseling.
There are a few people, such as progressive educators and
church organization members, who criticize the current
approach. They propose that we look to other countries for
West Germany
examples of possible alternatives. In Denmark, for instance,
there is something called "protected marriages"-houses are provided for mentally disabled couples so that they can live
together. Special attendants take care of their needs and the
needs of their children. The government provides these
services-Denmark is much more of a welfare state than West
Germany. Similar programs are planned in the Netherlands and
at least two similar programs exist in West Germany. Reports
indicate that these programs are highly successful. The main
drawback to the development of further programs is the lack of
available funding. This is a big issue in West Germany right now
as the social welfare law does not explicitly allow for funds to be
spent in this way. In addition, most of the disabled parents need
supplemental assistance as they earn minimal wages.
Until recently, disabled people in West Germany were
discouraged from having sexual relationships. Many books have
been published that state that the disabled should not have the
right to sexuality. In many institutions, methods were used to
distract disabled people from their sexual feelings. Although it is
currently said that the mentally disabled have a right to their sexuality, people are now trying to regulate the circumstances under
which the disabled are allowed to have sexual relationships.
There are some people who are supportive of the right of the disabled to sexuality. Several organizations offer services to disabled people who request reproductive counseling. They provide
advice on sexual problems and planned parenthood, and help
parents to educate their children about birth control.
The conservative West German government is trying to
pass a new custody law. There is a provision in that law that
states that for disabled people who are unable to give consent for
sterilization, the parents or legal representative have the power to
approve the procedure. The government wanted to enact this
law in September 1987, but was unsuccessful due to the resistance of the Green and Social Democratic parties. These parties
are very sensitive to this issue in part because of their work to
get compensation for Nazi sterilization victims. The Greens and
Social Democrats are supportive of the reforms in the new custody law except the provision dealing with the sterilization of
disabled people. The government had therefore excluded the
controversial provision in order to pass the reform of the custody
law. But the government will continue its fight to legalize the
involuntary sterilization of the disabled.
I think that one major problem is that many people believe
that the reproductive choices of disabled people are a public
issue and not a private right. There is also a prevailing attitude
that disability is abnormal and therefore unacceptable. If one
examines current developments in the fields of genetic engineering and reproductive technology, one can see that people have
(cont. on p. 28)
Connexions 25 Winter 1987
11
Restricted ''Choice''
Ireland
(Submitted by Pauline Ryder: The Dublin
Well Woman Centre, Dublin, Ireland,
October 1987.)
The Dublin Well Woman Centre was
founded in 1978 with the aim of providing
medical care, counselling, fitness programs,
and other services related to women's physical and mental well-being. Our philosophy is based on the principle that women
have the right to take control of their own
physical and mental health. In 1978, access
to family planning information was
severely restricted in Ireland. The Well
Woman Centre sought to help bridge the
gap between the limited services available
and the demand from Irish women for
easily accessible birth control. To date,
78,000 women from all over the country
have used our services. In addition, we
provide educational leaflets on aspects of
health including contraception.
Up until January, 1987, we provided
non-directive pregnancy counselling to
women coping with unplanned or
unwanted pregnancies. Our aim was to
create a safe, private, and accepting atmosphere in which a woman could discuss all
her options (including the option of abortion, which is illegal in Ireland). In cases
where a woman decided to have an abortion, we referred her to approved, legal
clinics in the United Kingdom. We also
acted as a telephone service for people
wanting information on abortion.
In October of 1986, a High Court
Action was taken against the Dublin Well
Woman Centre and Open Line (the only
other agency in the Republic of Ireland
offering this type of pregnancy counselling)
by the Society for the Protection of the
Unborn Child (SPUC). This action was the
result of an amendment to the Constitution
in 1983 which gave the foetus a right to life
equal to that of the mother. This amendment was sought by SPUC, which succeeded in winning the support of the main
political parties. The outcome of the High
Court case has resulted in an injunction on
our Pregnancy Counselling Service and the
closure of Open Line. Indeed, we are restricted by law from giving any information
concerning abortion. Recent statistics suggest that this injunction has done nothing
to reduce the numbers of Irish women travelling to England for abortions. The
injunction has pushed access to information underground (there is a national campaign which has set up a country-wide network). It has also increased the trauma and
stress women have to go through in order
to obtain an abortion.
The long term effects this will have
on women and their physical and mental
well-being are yet to be seen. It is currently
a civil offense to give out information on
abortion; women are made to feel like
criminals. We are being denied a basic civil
right-access to information.
12 Connexions 25 Winter 1987
We have appealed the High Court
decision to the Supreme Court, and are
awaiting the hearing. The legal fees
involved are astronomically high and the
success of our appeal depends on raising
the funds required to see the case through.
Any contributions to help us in our plight
would be most welcome.
Please send to:
Dublin Well Woman
73 Lower Leeson Street
Dublin 2
Ireland
(From Women's News, Irish women's
magazine, July/ August 1987, Belfast, Ireland.)
When the Society for the Protection
of the Unborn Child (SPUC) launched its
successful campaign to amend the constitution of 26 counties to guarantee the right to
life of the unborn, Southern politicians
assured us that this was not an attack on
women's rights, but merely an action to
prevent the courts from declaring the old
1860 Act (making abortion criminal)
unconstitutional. However, as many of us
feared at the time, the amendment was
only the first step in a much longer-term
SPUC strategy to deny women access to
information on both contraception and
abortion. In 1983, SPUC attempted to
intimidate women from seeking advice on
these matters by picketing family planning
centres and women's clinics. In 1986, they
went a step further and began a legal campaign to stop women's clinics from providing any services of this nature.
SPUC initiated court proceedings
against The Well Woman Centre and Open
Line Counselling. The case was heard by
Justice Hamilton, who found in favor of
SPUC; he ruled that all other constitutional
rights are held secondary to that of the
right to life of the unborn. The judgment
therefore denies women the constitutional
guarantee and equal right to life, the
guarantee to privacy, and the guarantee of
access to information.
Thus. from December 1986, nondirective
pregnancy
counselling
has
effectively been banned from twenty-six
counties. Furthermore, if the decision is
implemented literally, it would mean a distressed pregnant woman could not get
information on abortion from her closest
friend without potentially engaging in a
"criminal conspiracy." Doctors advising
patients on these matters could be
prosecuted. Certain contraceptives such as
the IUD and the morning after pill could
be banned. Popular newspapers and magazines could be censored. The fearsome
scope of the judgment and the danger it
poses for civil liberties has provoked an
angry response from women who are determined to defend their rights. It has also
brought the realization that SPUC must be
stopped now.
The Defend the Clinics campaign
began functioning as soon as SPUC's court
action was announced. The aim of the
campaign is to make the judgment against
the clinics unpopular and to create a network of information needed to restore the
challenged service. The Dublin-based
national committee has now distributed
hundreds of information packets (giving in
pamphlet form information previously
offered by the women's clinics), thus defying the injunction.
We believe that in order to succeed
in our campaign, not only must the
women's movement of the North and the
South unite, but all working class organisations, political parties, and progressive
forces in Ireland must fight SPUC's agenda.
If SPUC is not stopped, women will suffer
yet more defeats at the hands of the right
wing, and the outlook for the future of
Irish women will be unthinkable. □
Israel
(Submitted by Awatef Barghut,
clinic nurse, Nazareth, Israel.)
health
It is impossible to separate any subject in Israel today from the political and
social reality in which the economic crisis;
continuing occupation of the West Bank,
Gaza Strip and Golan Heights; the war in
Lebanon; and the continuing oppression of
Palestinian people are major factors. With
respect to abortion, women's reproductive
rights are limited. In order to have an
abortion in Israel, a woman must appear
before a committee consisting of a doctor,
psychologist and social worker, and receive
their permission. The only grounds for
approval are if there is severe danger to
mother or child, if the pregnancy is a result
of rape or incest, if there are special religious reasons, or if the mother is mentally
incompetent. The "social clause" of the law
permitting abortions for socio-economic
reasons, by which most abortions were performed in the past, was cancelled in 1978.
I can't say that there is a policy of pressuring Arab women to abort, but people say
that despite the law, all Arab women can
get an abortion when they request one, as
opposed to Jewish women, who are pressured to have the child. Jewish women are
told they can put the child up for adoption
if they don't want to raise it. □
India
(From Manushi, Indian feminist monthly,
no. 36, 1986.)
Abortion in India was legalised in
1972. The number of legal abortions is
increasing steadily each year. Unfortunately, the number of illegal abortions
performed is also increasing. The increase
has occurred through sustained propaganda. People have been led to believe
that abortion is a trivial operation. It is
often advertised as something that is cheap
and easy to have done on your lunch
break. Abortion is projected as a procedure of little financial or physical consequence.
Commercial
interests
have
encouraged many illegal practitioners to
perform abortions.
Many people see abortion as a simple
procedure that a person with any sort of
medical
qualification-allopathic,
ayurvedic, or homeopathic-is competent
to perform. It is even said that non-medical
persons can easily learn the technique. In
spite of all the modern and safe methods of
terminating pregnancy that are available in
this country, severely damaging and often
ghastly methods continue to be used to
induce abortion. A spate of reports in the
last two years reveal that iron nails, sticks,
coconut splinters, and Fetex, a dangerous
chemical paste, have all been used by illegal abortionists. The types of injuries
inflicted by illegal abortionists are horrifying. Perforation of the uterus and injury to
the rectum , urinary bladder, intestines and
liver, severe infection of the peritoneum .
and chemical burning and sloughing of
internal organs have all been reported in
recent cases.
The havoc caused by septic abortions
continues unabated in spite of all the
powerful infection controlling drugs available now. There are no beds earmarked for
abortion cases in hospitals. Centres for
medical termination of pregnancy have to
be approved by medical authorities, but
many unapproved centres continue to function.
A report from Patna Medical College
Hospital reveals that maternal deaths due
to abortion have increased from 5.6 percent of all maternal deaths between 1961
and 1965 to 9.0 percent between 1976 and
1980. Fetex chemical paste, licensed, publicised and popularised as an abortificent
paste, has caused peritonitis, gangrene of
organs and kidney failure in many cases.
Doctors recommend that advertisements
for Fetex paste should be banned and the
product withdrawn from the market. It is
due to the inefficiency of the mechanism
for controlling drugs in our country that
after years of reporting on the fatal effects
of this paste, it continues to be licensed
and marketed. D
Hong Kong
(From Women's News Digest, June-August
1986, Hong Kong.)
The approval of two registered doctors is required for a legal abortion under
the present Hong Kong law. This law
denies women the right to make decisions
about their own bodies by allowing doctors
to impose decisions on them. Therefore,
the legal system in Hong Kong is forcing
women to cross the border into China to
seek cheap and easily accessible abortions.
In addition, the laws have contributed to
the number of women seeking illegal abortions from unlicensed doctors in Hong
Kong.
Ms. Chan, chairwoman of the Association for the Advancement of Feminism,
believes that the trend of seeking abortions
across the border is "a result of the
insufficient abortion service in Hong
Kong." Medical and Health Department
statistics show there were 28,130 legal
abortions between January 1982 and
December 1984. Among these, 70.8 percent were carried out in private hospitals,
while only 7.2 percent were carried out in
government hospitals. Just over 22 percent
were carried out in subsidised hospitals.
Ms. Chan points out that "The fact that a
high percentage of women are having to
terminate their pregnancies in private hospitals indicates the inadequacy of a cheap
abortion service." She goes on to report
that middle and upper class women have
easy access to abortions because they are
able to pay the cost, usually between
$3,000 and $5,000. Lower middle class
women are often obliged to seek cheaper,
but more dangerous illegal abortions.
"The only other viable alternative
seems to be the service available across the
border, despite the possible risks due to
lack of follow-up service." "A strong
stigma attached to pregnancy out of
wedlock shames women into getting abortions, whether they want their children or
not." It is this stigma which drives many
women, especially young women, across
the border for abortions.
Ms. Chan states that it is necessary
to challenge and change the hostility
against unwed mothers. As a more immediate task, however, she stresses the need to
provide sex education and information
about contraception to women, a task
which a responsible government cannot
ignore. D
Mauritius
(From "Medical Guide-Illness No, Health
Yes," and "Women's Minimum Program,"
Mauritius.)
"One child is enough, and it matters
little whether daughter or son, as long
as the child is healthy and strong.,,
According to the Penal code section
235, abortion in Mauritius is illegal. The
law originated in the colonial period and
should be immediately revoked in order to
decriminalize women. This is all the more
necessary because according to statistics,
every woman in Mauritius has an average
of five abortions within her lifetime.
g According to government figures, four
6 thousand women are hospitalized each year
~ as a result of clandestine abortions. Doctors estimate that approximately 40,000
women each year have an abortion, many
of whom seek cheap abortions. Unfortunately, these inexpensive abortions are
often done with utensils such as umbrellas,
knitting needles, or spokes causing many
women to suffer from complications that
can be terminal. Among the points listed in
the Women's Minimum Program, which
the Women's Liberation Movement distributed to all the major parties, was a
demand to repeal the Penal Code Section
235 immediately. □
Connexions 25 Winter 1987 13
Japan
(From Asian Women's Liberation, Japanese
feminist quarterly, No. 6 1984.)
Nineteen eighty-three was a crucial
year for women in Japan. The Ministry of
Welfare proposed legislation aimed at
tightening restrictions on abortions. The
course of events began in March, when
Representative Murakami Masakuni, who
is backed by right-wing religious groups,
announced: "Vast numbers of abortions
continue to be performed for economic reasons despite the fact that Japan has become
an economic superpower. This casts doubt
on the future prosperity of the Japanese
people. Abortion is murder. Allowing it to
continue unchecked will result in the moral
degeneration of our society. Accordingly,
abortion must be strictly controlled."
The first step toward this end was to
propose deleting the "economic reasons"
provision from the list of conditions contained in the Eugenic Protection Law
under which a woman may obtain an abortion. Proponents of the revision launched a
huge media campaign and held rallies using
such slogans as "Respect for Life" and
"Protect Fetal Life." They also methodically collected over ten million signatures
to a petition calling for the revision,
including those of legislators from all levels
of government.
The fundamental law in Japan concerning artificially induced abortions
prescribes imprisonment for women who
procure unauthorized abortions. Other provisions prescribe varying penalties for doctors, midwives, pharmacists, druggists and
others who participate in such abortions.
These provisions were first introduced to
the criminal code in 1880 as part of the
westernization Japan was undergoing at the
time. Previously, abortion had not been
treated as a legally punishable offense. In
fact, during the years 1603 to 1868, both
abortion and infanticide (which was often
sex selective) were routinely practiced by
poor rural peasants as a form of self preservation and a method of population control.
(As a result, the overall population
remained stable for almost 300 years.)
The criminal abortion laws introduced in 1880 were significant in that they
coincided with a new national policy to
westernize Japan in terms of wealth and
military strength. One aspect of this policy
called for boosting the country's population . Especially from around 1930 until
1945, women's bodies became the territory
of the state. Motherhood was a public duty;
the criminal abortion laws were strictly
enforced and even contraception was forbidden. The first priority was to ensure a
supply of labor and soldiers for the war
effort.
In 1948, the Eugenic Protection Law
was introduced. Its purpose was to control
the enhancement of desirable Japanese
racial qualities primarily through sterilization and abortion. The conditions under
which abortion can . be performed are
divided into three major categories: {I) for
eugenic reasons (existence of hereditary
physical or mental disorder); (2) for public
policy reasons (pregnancy resulting from
rape or coercion); and (3) for personal
14
Connexions 25 Winter 1987
sociological reasons (possible injury to the
woman's health from a physical or
economic viewpoint). Economic reasons
were added to these conditions as a new
category in 1949. In effect, this had led to
the realization of abortion on demand in
Japan. These demands are sometimes
based on fictitious claims of economic
hardship.
Japan's population needs changed
dramatically following World War II. Having lost its foreign territories and facing
acute food shortages, reducing the population became a national priority. Also, in
order to alleviate the increasing number of
back-street abortions and the physical
dangers these presented for women, it
became necessary to legalize abortion.
There can be no doubt that the reduction
in the size of Japanese families after the
war can be primarily attributed to abortion.
native intelligence. They worry that among
those fetuses "selfishly" aborted there may
have been geniuses who might someday
have benefited Japan's economy.
It is not enough simply to have this
offensive bill shelved. The opposition
movement is starting to prepare its own
reform proposals. Feminists have been trying to abolish the Criminal Abortion Law
and the Eugenic Protection Law altogether.
The Criminal Abortion Law is an
unjustifiable governmental intervention
into individual privacy and ignores basic
human rights. The Eugenic Protection Law
is premised on the philosophy of promoting racial purity. The net effect is to deny
women through forced abortion the opportunity to have children when they want
them, and to penalize women who choose
to terminate unwanted pregnancies. It is
important that we work for an environment which enables women to choose
One bill to revise the Eugenic Protection Law was introduced in 1972, during
the last stage of Japan's period of high
growth immediately preceding the oil
crisis. The central feature of the bill was
the deletion of "economic reasons" and its
replacement by the purely medical condition of "mental or physical health reasons." Abortion would also be allowed
where the fetus was found to be handicapped. The bill also required young
women who had never given birth to
receive advice and guidance before an
abortion could be performed. A key factor
said to be behind the bill was the shortage
of young workers to meet the demand for
labor caused by Japan's high economic
growth. From this need emerged the
national priority of increasing the country's
human resources. The bill was met with
intense opposition and was successfully
blocked in 1972 and 197 4.
In 1982, reflecting Japan's increasingly conservative political climate, the
proposal to strike "economic reasons" from
the Eugenic Protection Law once again
came to light. Conservatives say that Japan
lacks the necessary natural resources for
economic development; therefore it is crucial to utilize Japanese people's "superior"
whether or not to have children, so that
men and women together can achieve their
full potential as human beings. Contraceptives are very tightly regulated by the
government in Japan, therefore, the first
priority should be to provide better contraceptive planning and services for couples
who choose not to have children. □
Contact:
• Muvman Liberasyon Fam, Lakaz Ros, 8
celicourt Antelme Street, Forest-Side, Mauritius.
• Defend the Clinics Campaign, National
Committee, 6 Crow Street, Dublin 2, Ireland.
• The Women's Centre for Advice and
Information, 18 Donegall Street, Belfast,
Ireland.
Further Reading:
• "Irish Women Defiant Over Abortion
Rights," Out write, British women 's newspaper, Issue #55, February 1987.
• Women's News Digest, Association for
the Advancement of Feminism, Hong Kong,
June-August 1986.
The International Meeting on
Women and Health
Costa Rica
(From "The International Meeting on
Women and Health," by Maria Eugenia
Jelencic, Women in Action, an Isis International publication, 1987/2.)
About 800 women from five continents met in San Jose, Costa Rica last
May for the Fifth International Meeting on
Women and Health. The week-long meeting was organized by the Feminist Center
of Information and Action (Centro Feminista de lnformaci6n y Acci6nCEFEMINA) of Costa Rica. There was a
large representation of Costa Rican women
and Latin American women in general there were very few Asian women (about
20) and even fewer African women (no
more than l 0).
The Women and Health Movement
has developed appreciably since 1977, the
year of the First International Meeting on
Women and Health in Rome, Italy. For
· many groups and organizations, it was the
first time they had encountered women
from different countries doing work similar
to their own. The San Jose meeting was a
demonstration of the vitality of the movement. There were three central workshops:
"Reproduction Rights and Population
Problems," "Medicines and Drugs," and
"Community Health," and 130 other
workshops were proposed by the various
groups who took part in the meeting.
The initial program had to be
modified and adjusted several times in
order to allow a forum for each problem.
First there were the specific, daily problems
which confront women as a gender. In the
majority of the countries represented,
women's groups are the only place where
these problems can be confronted. The
titles of the following workshops are indicative of the issues that women's groups
take on: "Circumcision of Women in
Sudan," "Women Under Muslim Law,"
"Mental Condition and Female Condition," "Physical and Mental Illness in
Women as Resistance to Patriarchy,"
"Alternative Sexual Education," "Subjected Body/Despised Body," "Effects of
Drugs on Lactation," "Psychosocial Elements of Maltreatment of Women," "SelfHelp Groups," "Domestic Violence" and
many others. There were also workshops
on environmental pollution, the Chernobyl
and Bhopal disasters, and on abuses of the
new reproductive technologies.
It was generally agreed that the
women's
health
movement
must
significantly increase its organization and
reinforce itself as a pressure group that can
promote political change. There is a lack
of adequate instruments of communication
and of materials with content that
effectively supports health programs. The
dissemination of information to illiterate
women, especially in the rural sectors and
inner cities of the Third World must be
addressed, as lack of information is the
basis of much abuse: forced sterilization
and the use of poor women as "guinea
pigs" in experiments with contraceptives
are just some of these violations.
Isis International is working on
improving the communication of health
information to all women. In the workshop
"Audiovisual Communication as Support
for Women's Health Programs," which Isis
coordinated, several groups were cited for
making progress in this area. One of Isis's
own projects is a low-to-medium cost training workshop for health workers in groups
in the Latin American region. Ana Maria
Portugal of Peru told of a network that has
been initiated in her country to provide
audio cassettes containing programs for
women. Ilet Mujer is also promoting a
Latin American radio network, and in
India, there have been seminars in video
training for Asian activists.
The groups which participated in the
workshop on the Health Network of Latin
American and Caribbean women indicated
how valuable the creation of this network
had been in breaking the isolation of
groups working at the local level, and how
it had also helped towards coordination at
a regional level. This network started in
1984 and now includes 500 organizations
and groups in the region.
The workshop of the Global
Women's Network on Reproductive Rights,
which includes about 600 groups, was
another confirmation of the effectiveness of
the networks. "When we began to coordinate with other Asian groups we discovered
that many of the population control policies which were being implemented in
India were the same ones that exist in
other countries in the region," said one
representative from Saheli, an Indian
organization.
One great concern for women
involved in the reproductive rights movement is drug dumping. "Through the network, solidarity and vigilance among
women can be intensified," said one participant in the workshop on Drugs and
Medicines. "If we are better coordinated,
women in developed countries can exert
pressure to make sure that medicines and
contraceptives which are prohibited in
those countries are not sold in Third World
countries as they are today." In a final
document, signed by the Third World
women present at the conference, severe
criticisms were made of the majority of
health policies implemented in their countries.
One section of the document reads,
"Health policies implemented in our countries are based on profits and on power for
elites ... Added to this is the deterioration of
the economic situation of the developing
countries as a consequence of International
Monetary Fund tax policies, which are the
cause of poverty, hunger, unemployment
and lack of housing. In consequence, serious health problems for millions of people,
especially women, are created." The situation is complex. Can support for the
Women and Health Movement help to
improve the situation? Do we help to
improve the situation? We think so. In
many places the Women's Health Movement is still in its initial stages.
In the next meeting, planned for
1989 in the Philippines, it will be possible
to evaluate all the advances achieved in
these two years of work. However, in the
meantime, we must keep in contact, tighten
our bonds and work in a coordinated way.
There is no other way to achieve significant
advances. □
Contact:
• Centro Feminista de Informaci6n y
Acci6n, Apdo. 5355, San Jose, 1000 Costa
Rica.
Further Reading:
• "Conference Demands International
Health Rights," Outwrite, British women's
newspaper, Issue 60, July/August 1987.
Marie Falksten ©
Connexions 25 Winter 1987
15
Nigeria
AIDS Linked to Genital Mutilation?
(Submitted to Connexions by Hannah
Edemikpong, coordinator of the Women's
Centre in Nigeria.)
The question of where the AIDS
virus originated is a matter of intense
international debate. Some say that AIDS
may have appeared first among the green
monkeys of Central Africa or perhaps in
some backwater village in the interior of
the continent. Whatever the outcome of
the international debate, it is indisputable
that AIDS is here and is spreading ram•pantly. Seldom has a single disease put so
many people around the world at great
risk. The AIDS microbe comes in a variety
of strains and has the ability to mutate
rapidly, making the development of potential vaccines highly problematic.
16 Connexions 25 Winter 1987
Some scientists say that as many as
five million Central Africans may carry the
virus. The World Health Organization says
that the virus is now spreading to other
areas in Africa. The overwhelming majority
of Western victims still come from two
specific groups: male homosexuals and
intravenous drug users. But what is happening in Africa is quite a different story.
What are the cultural factors involved in
the transmission of AIDS in Africa? Uli
Linke, an anthropologist and researcher at
the University of California, Berkeley, says
that there is "a prevailing assumption that
the same cultural factors are at work in the
transmission of AIDS in Africa as in
Europe and the USA. .. But none of the cultural factors can explain the equal ratio of
men and women contracting the virus in
Central Africa. The bottom line in the
transmission of AIDS is the exchange of
bodily fluids, particularly blood, which
gave me the idea that it might be related to
female circumcision."
In Africa, women are noted carriers.
In a recent survey done in Uganda, of the
170 pregnant women tested, 75 percent
were found to have AIDS. Half of those
found to have AIDS had been genitally
mutilated. In Equatorial Guinea, of the 100
women who were tested, 78 of them carried AIDS and 65 of them had been genitally mutilated.
The forces that make people subject
girls to genital mutilation are varied. Sexual, religious, and sociological reasons are
often cited as causes. Some African
societies believe that the operation diminishes a women's sex drive. The decrease in
women's sex drive is sometimes ignorantly
believed to decrease the incidence of prostitution. Some religions, such as Islam,
advocate female circumcision. In some
parts of Nigeria, circumcision is a rank of
honour and distinction for both the girl
and the family. In Egypt, for example, the
uncircumcised girl is called 'Nigsa'
(unclean). Western efforts to eliminate the
practice through missionaries or colonial
masters have forced people to hold on to
their cultural traditions for fear of being
exposed to the ill effects of Western
society.
The most extreme form of female
circumcision, infibulation, is the complete
removal of the vulva! tissue including clitoris and the labia. After the tissue has
been removed, the sides of the wound are
sewn together. This leaves a miniscule
opening about the size of a matchstick. No
anaesthetic is used and the instruments are
not sterilized. [editor's note: Female circumcision can be done in groups, therefore
the sterilization of instruments is essential
in preventing the transmission of AIDS.]
Essentially, sexual intercourse is impossible
unless the vagina is reopened. This is often
done through forcible entry by the husband, which can lead to hemorrhaging. In
women, "infibulation is associated not only
with chronic pain, but with lesions in the
vaginal tissue which lead to the presence of
blood during intercourse," says Linke. He
further states that "it is noteworthy that
the recent outbreak of AIDS in Africa
corresponds geographically to those regions
in which female genital mutilation is still
practiced." We, at the women's centre, are
extremely concerned about the rampant
spread of AIDS and its connection with
female genital mutilation. We have
launched an educational campaign to
inform women about the situation by home
visits, newsletters, and public speaking
events. As a non-governmental voluntary
organization without a solid financial base,
the greatest problem in our ongoing campaign is funding. Any donations would be
greatly appreciated. Please help us to stop
female genital mutilation and the spread of
AIDS among African women. □
(From the International Symposium on AIDS in Africa,
Naples, Italy, October 7-9, 1987. )
Uganda:
1983 I 7 AIDS-cases
1987 I, 138 AIDS-cases
1987 6% of prostitutes are HIV-positive
Rwanda:
1981 10 AIDS-cases
1987 705 AIDS-cases, (246 are children)
Zaire:
I 987 6-8% of pregnant women are HIV-positive
1987 I 1% of prostitutes are HIV-positive
Congo:
1987 583 AIDS-cases
Kenya:
I 985 6 I% of prostitutes are HIV-positive
Tanzania:
198 7 1130 AIDS-cases
Cameroun:
1987 1.5% of pregnant women are HIV-positive
Ghana:
198 7 96 AIDS-cases
Senegal:
1987 14% of prostitutes are HIV-2-positive
Guinea-Bissau:
1987 60% of prostitutes are HIV-2 positive
Tunisia:
I 98 7 11 AIDS-cases
Contact:
• Ministry of Health
P.O. Box 30016,
Nairobi, Kenya
Further Reading:
• Report on AIDS, by the Panos Institute, 8 Alfred
Place, London, WClE 7EB, UK.
• The Politics of AIDS, 1he New Internationalist,
No. 169, March 1987.
• AIDS Acti on, (International newsletter fo r AIDS
info rmation), Published by AHRTAG, 85 Marylebone
High Street, London, WIM JDE, UK.
Contact:
• Hannah Edemikpong, Women's Center,
P.O. Box 185, Eket, Cross River State,
Nigeria, West Africa.
Further Reading:
• The Circumcision of Women, By O/ayinka Koso-Th omas, Z ed Books Ltd. , London 1987.
Connexions 25 Winter 1987
17
India
Cooking Inside
-The Effect of Wood Smoke on the Health of Women
(Excerpted from an article by Anil Agarwal
in Manushi, an Indian feminist monthly,
no. 28, 1985.)
Atmospheric pollution has long been
regarded as probably the least important of
all the environmental problems in rural
areas, a problem which is concentrated
mainly in major cities and industrial
towns. But recent evidence shows that air
pollution within homes may be an acute
problem, an underlying cause of millions of
deaths every year. The burning of cooking
fuel envelops the indoor environment with
heavy smoke, and women, who have to do
all the family cooking, may be daily
exposed to more pollutants than even
industrial workers in extremely polluted
environments on smoggy days.
For thousands of years, people have
cooked using firewood and cow dung.
Even today, over 90 percent of households
use wood, dung and crop residues as fuels.
Environmental protection agencies in
developed countries commissioned a
number of studies to assess the impact of
firewood use on air pollution. These studies revealed that biomass fuels, particularly in small scale combustion as in
residential stoves, emit several important
pollutants in high quantities compared to
gas, oil, and even coal-the most polluting
fossil fuel.
18
Connexions 25 Winter 1987
But what about homes in a country
like India where cooking is commonly done
on open and inefficient chu/has with few
arrangements to funnel the smoke out of
the house? A pilot study in four villages of
Gujarat was carried out in late 1981. The
woman cook in each household was asked
to wear a sophisticated air sampler which
was clamped to the collar, so that the
measurement device could move around
with the cook and measure her actual exposure to major pollutants in wood smoke.
The results were shocking. The average exposure of women to the pollutants
was over fifty times greater than the safety
levels set by the World Health Organisation. Women cooks receive a larger total
dose than would residents of the dirtiest
urban environment. Even an industrial
worker would rarely be exposed to the levels found in the Gujarat study.
A number of factors make the level
of exposure to pollutants worse. Dwellings
in villages are small and badly ventilated.
In one of the Gujarat households, when the
holes in the roof were closed, as is done
regularly in monsoon conditions, ventilation was so reduced that it became impossible for the researchers to remain in the
kitchen for more than a few seconds
because of the discomfort caused by heavy
smoke. The woman cook, however, stated
that such conditions were normal during
the monsoon.
What does this mean for the health
of women who cook? The most powerful
evidence for the ill effects of wood smoke
comes from a survey of a heart disease
called cor pulmonale, in which the right
lower chamber of the heart enlarges and
fails because of a disorder in the lungs. The
survey was carried out over a period of 15
years on hospital patients in Delhi. The
authors, Dr. S. Padmavati and Dr. S.
Arora, concluded that because of the fact
that women are exposed to smoky primitive fireplaces from early ages, domestic air
pollution accounts for the higher prevalence of cor pulmonale in women than in
men.
In Ahmedabad, another study of the
incidence of cough, cough with expectoration, dyspnoea (difficulty in breathing) and
lung abnormalities, found a statistically
higher incidence among women cooking
with smoky fuels. Furthermore, studies in
Nepal have shown a strong association of
domestic smoke with chronic bronchitis.
Exposure to carbon monoxide (CO),
a colourless and odourless gas which is
highly toxic if inhaled in sufficient quantities, is also a health problem for Indian
women. Evidence points to a strong link
between chronic CO exposures and both
heart disease and impaired fetal development. Recent evidence points to a strong
association of CO with heart diseases.
Any condition which results m
reducing the blood's capability to carry
oxygen to the tissues, like anaemia, will
also make a person more susceptible to carbon monoxide toxicity. This is particularly
bad for Indian women, who are anaemic in
large numbers. Chronic lung diseases will
further reduce the capability of the blood
to rid itself of carbon monoxide during
periods of low or no exposure. There are
several factors that make women particularly susceptible to CO exposure. Women
generally have less haemoglobin reserve
than men, which makes them more prone
to anaemia, and also makes them more
vulnerable to lower doses of CO than men.
During pregnancy, there is additional
demand on haemoglobin, further lowering
their reserves and making them even more
sensitive to CO. This exposure can also
affect the unborn child, leading to reduced
birth weight and increased perinatal death
rates. It is not surprising that respiratory
diseases are a leading cause of death among
women and girls over the age of five in
India.
Women begin cooking as young girls
and continue for much of their lives.
Young girls may receive significant exposure at their mothers' sides even before the
often tender age at which they begin cooking full time. In the case of cooking smoke,
inhalation is inevitable because exposure to
smoke comes with every breath. Pregnant
and nursing mothers generally have no
option but to cook and so remain exposed
to smoke.
There is general agreement that the
health of rural women is significantly worse
than that of the rural male population. A
number of reasons have been presented to
explain this phenomenon: high fertility
rates, less access to health care, inadequate
diets, and differences in economic roles.
Smoke exposure could also be one of the
major factors.
There are many steps to be taken
that will cut down the exposure to smoke
and reduce its adverse impact on women's
health. One aspect of the wood smoke
solution is to increase ventilation in the
homes of the poor. Ventilation improvement could be the least expensive, shortterm way to reduce smoke exposure.
Unfortunately, house designs are usually
decided by the males in the house who do
not spend endless hours cooking under
these horrid conditions. In addition, certain species of trees known to give off less
smoke when burnt should be grown in special forestry programmes.
Improved stoves are also a key factor
in solving the problem. The new Nada
stove, which former architect Madhu Sarin
helped to pioneer, evolved spontaneously
out of the traditional stove in the village
when Sarin worked closely with the stove
users. Sarin works closely with the
beneficiaries of the new technology, even at
the design stage. For Sarin, involvement of
women in stove dissemination programmes
is crucial. She argues that women seldom
make decisions even about their own technological needs and the little cash that
would be needed to purchase new technologies is denied to them by men. Thus, stove
dissemination programmes must be undertaken in a way that they support and
increase the confidence of rural women.
Sarin is today the most successful disseminator of improved stoves in India.
There are serious implications for
health policy planners in these findings.
Just as supply of clean water is now considered an extremely important domestic
need in the rural areas, the supply of clean
air is also a matter of high priority for
rural women. D
Further Reading:
• Looking at Appropriate Technology,
Women's World, an Isis International publication, Geneva, Switzerland, June 1986.
Connexions 25 Winter 1987
19
The earth's population is now over
five billion. The majority of these people
live in developing countries where the quality of the water supply and sanitation is
poor. The World Health Organization estimates that 80 percent of human sickness
and disease in developing countries is
related to inadequate water supply and poor
sanitation. The United Nations therefore
declared that the decade of the 1980s would
be devoted to providing these countries with
adequate water supply and sanitation.
Where water quality and sanitation
are problematic, women are greatly affected.
Some Third World women expend up to 27
percent of their caloric intake through the
heavy work involved in transporting water.
This work causes more than fatigue-pelvic
disorders and complications at childbirth
are often a result. In addition, mothers must
contend with the fact that children are
disproportionately the victims of water- and
sanitation-related diseases. For example,
water-borne diarrhoea illnesses kill over five
million children in developing countries
each year. Other water-related illnesses,
such as parasite worms and cholera, also
claim many children's lives. Because of
women's special role with regard to water
supply and sanitation, it is imperative that
women be actively involved in all aspects of
planning and implementing water projects.
20 Connexions 25 Winter 1987
Kenya
Water:
An Obstacle for African Women
(Excerpted from a talk by and subsequent
interview with Bibi Hamisi, an extension
worker with the Kenya Water for Health
Organization and Hilda Paqui, a United
Nations Development Program Information Officer from Uganda. Recorded for
Connexions on Nov 2, 1987.)
Q: How has the Water Decade affected the
world population?
Hilda: Due to efforts associated with the
Water Decade, 345 million people have
gained access to clean drinking water and
about 170 million have gained access to
better ways of disposing of their waste products. But because of population growth,
the number of people without access to
clean drinking water at the end of 1985
was the same as in 1979; so we have hardly
made a dent. Without the projects of the
water decade though, the situation would
obviously be much worse.
Q: Besides population growth, what are the
other factors which negatively affect water
supplies and sanitation?
Hilda: Shifting populations, for one; due to
migration, fifty percent of the Third World
population will soon be living in urban
slums. While water and sanitation are often
poor in rural areas, it is even more difficult
to find solutions for people living in urban
slums and squatter settlements.
Q: What role do women play in this
scenario?
Hilda: In 1986, the United Nations
resolved that attaining self-sufficiency with
regard to food is a top priority in order to
help Africa eliminate its current economic
bind. In Africa, women are responsible for
80% of the food production. Therefore,
unless we release women's time and energy,
this goal cannot be achieved. In rural
Africa, women must put forth tremendous
efforts in order to obtain water. For
instance, in Burkina Faso during the dry
season, women walk to distant water
sources after sunset, sleep there, and then
return at dawn carrying 25 kilos of water.
You can imagine how physically exhausted
a woman must feel after spending at least
seven hours collecting water and also after
having slept outside. She will have little
energy to work in the garden, grow and
process food, take care of her family, or
generate income. She certainly won't have
time to take care of herself. It is also
important to train women in agricultural
methods and to obtain better seeds and
farming tools (for which financial credit is
necessary). But time and energy is the most
crucial factor in African women's lives. If
they do not have the time, they cannot take
advantage of training and improved farming equipment.
Q: In which project are you involved?
Bibi: We train women to maintain newly
installed, hand-operated water pumps. My
major role in this project is to train and
mobilize the community.
how to make deposits and withdrawals
from their banks. Then we hold workshops
to train the women in water pump maintenance. After the women learn how to
assemble and dismantle the pumps, they
get a chance to practice out in the fields
and to train other women to maintain the
pumps. We do follow-ups to see how they
are doing. If they are successful, we finally
provide them with a pump. So far, we have
provided pumps for fourteen communities,
and they are being run well.
Q: How did this project get started?
Bibi: Before the water pumps were
installed, women had many health problems. Women had to walk four or five
kilometers away from home in search of
water. The little water they do find is often
contaminated. In 1979, we had an outbreak of cholera. The situation was so bad
that in 1983 the Ministry of Water
Development came up with a plan for providing clean water to help communities
control such diseases; the Ministry drills
boreholes and we mobilize and train the
community. The real challenge of providing villages with water does not lie in drilling wells and installing pumps, but in
making sure that the pumps continue to
work properly. The community must be
trained to do preventive maintenance and
to properly care for the pumps, if the project is to be successful.
Q: How do you involve local communities?
Bibi: Before a drilling, community
members consult with us about the water
availability in their area. After that, we do
a household survey to find out how many
permanent residents there are in that area.
There should be a well and a pump for
every 125 residents. Otherwise, they will
break frequently from overuse. Then, the
community members form water committees whose purpose is to make suggested
improvements about the project. We
require the community members to contribute money to the project in proportion to
their incomes. They get together to discuss
how much to contribute either on a daily,
weekly or monthly basis. They also select a
secretary, a treasurer and a chairperson,
who are in charge of financial matters.
These three people are usually women, particularly the treasurers. We show them
UNICEF/Bernard Pierre Wolff
Connexions 25 Winter 1987
2I
Q: What has led you to give priority to
training women?
Bibi: The men are not trustworthy. We had
a lot of problems when men took care of
the money. For example, in one community we suggested that they get a box in
which to store contributions. Although the
box could not be opened from the outside,
the men found ways to crack it open. That
was really upsetting! Our experience in
Kenya shows us that men are interested in
money more than anything else. Often
they care little about the welfare of their
own families. Sometimes families have to
live without husbands and fathers for
several months. We have found that it was
of no use to train men to look after pumps
because problems would occur, and the
man in charge would not be there to take
care of them. At one point, the men in the
community corriplained that we were
selfish; they wanted us to include more
men in the training. We did not want to
show them that we did not like them. We
have had to begin choosing one man for
each training session so that they would
feel recognized. Currently, one man and
five women maintain each pump.
Q: Who elects the maintenance workers?
Bibi: The communities do. We want them
to choose their own people because they
know who is good.
Hilda: When the villagers select women to
train for hand pump maintenance, there
are certain criteria they use. For example,
they might choose somebody who lives
closer to the well so that she can walk over
to the water pump with her children.
Q: Are you working with different women's
groups?
Bibi: Oh yes, we work with fundraising
groups. First, they register themselves, then
they find a way of generating some income.
Q: Have women's roles and status been
improved by their involvement in the
maintenance of the water pumps?
Bibi: Oh yes, of course, especially because
women now engage in income generating
activities. Some groups have even started
building shops for grinding machines. People walk ten to twenty kilometers to use
their grinding machines.
Hilda: When I visited Bibi's project two
years ago, another thing the women were
doing was growing vegetables around water
pumps-using run-off water. By doing so,
they can sell the vegetables and raise
money for pump maintenance and, in five
or ten years, pump replacement. Growing
and selling vegetables in the community
also helps improve community nutrition.
So water pumps have all kinds of spin-off
advantages.
Q: In what other ways has the installation
of water pumps affected the health of the
community?
Bibi: Well, cholera has been eradicated. We
have fewer cases of bilharzia. Malaria has
remained a problem because there is still
stagnant water-it is not spread by drinking
water. Diarrhoea is also less of a problem.
22
Connexions 25 Winter 1987
Q: What about sanitation?
Bibi: We are in the process of implementing a project that improves sanitation. The
Ministry of Health provides the labor, the
communities provide the construction
materials, and we coordinate the activities
of the Ministry and the communities. They
have started to construct pit latrines in
public areas, such as the health center,
mosques, schools, and markets; in some
villages groups of ten to thirty people are
digging pit latrines for every household.
We are trying to use local materials in the
construction of the latrines. Local materials are inexpensive. In addition, community members are involved in the construction; thus they have an investment and
they also acquire the expertise to maintain
the latrines properly. But most importantly,
this project, like the provision of water
pumps, is improving the health and well
being of the women of Kenya. □
Contact:
• International Drinking Water Supply
and Sanitation Decade, Hilda Rwabazaire
Paqui, United Nations Development Programme, Room DCl-1902, One UN Plaza,
New York, NY, 10017.
Further Reading:
• "Women and Water," Women's World,
an Isis International publication, Geneva,
Switzerland, June 1986.
• "Water Well," Connexions #6, Fall 1982.
• "Women, Water, and Donkey Work,
Kenya," Women's World, an Isis International publication, Geneva, Switzerland,
December 1986.
Canada
Women and Substance Abuse
(Translated from an article by Marie-Claire
Dumas in La Vie en Rose, • a Canadian
feminist monthly, October 1986.)
Two hundred women gathered at a
1986 conference entitled "Women and
Drug Addiction" in a town north of
Toronto, Ontario. Women addicts and exaddicts themselves were the main participants. Most of these women were searching
for help-not only with their addictions,
but also with the pain that has in so many
cases been responsible for the onset of their
addictions. All kinds of drug abuses were
addressed, from heroin and cocaine to
tobacco and alcohol.
Alcoholism is now having a profound
effect on young women, single women, and
women who live and work in large cities.
For these women, alcohol works as a
mechanism to help relieve the stress that
comes
when
they
don't
receive
"compensation-financial, psychological, or
social-that is their due." Women who are
especially at risk are those working in jobs
that are menial, repetitive, and low-paying.
They face constant battles against low selfesteem and the frustration that comes from
doing monotonous work. Since these
women have little or no support network,
their negative feelings can be repressed, at
least temporarily, by drinking alcohol.
Unfortunately, alcoholism in Canada is the
third leading cause of death among women
ages 33 to 55 (Women's Health).
The other "legal" addiction which is
having a devastating effect on the women's
community is tobacco addiction. Cigarette
smoking has been increasing among women
since the 1960s. In contrast to previous
studies, it is now reported that in the 12 to
19 age group there are more girls smoking
(25 percent) than boys (20 percent). There
are many factors which can account for
this historical change. Studies have shown
that cigarette smoking is associated with
the repression of negative emotions such as
anger and anxiety. Unfortunately, women
are often discouraged from expressing these
negative emotions, and then turn to
cigarettes for a release from frustration. In
addition, ever since the late 1960s,
cigarette smoking has been commercialized
as an empowering tool-a habit which
signifies women's equality with men. The
tobacco industry portrays women smokers
as self-assured, strong, and confident. But
what the tobacco industry does not tell us
is that women in Canada are dying in
record numbers from lung cancer and other
diseases caused by cigarette smoking.
Women must pay particular attention to the risks of drug addiction, says
Louise Nadeau, a toxicologist at the
University of Montreal. She believes that
women are more at risk because of the
nature of women's role in society. The
characteristics of the feminine role-selfsacrifice and subservience to others-have
brought about a feeling of loss of control
over the environment. This loss, she says,
"plays an important role in the distress so
uniquely felt by women, a distress manifested in certain cases by depression, anxiety, and the use of mood-altering drugs."
Another factor which often plays a
part in women's addictions to drugs is sexual abuse. Statistics indicate that violence
and sexual abuse have been part of the
lives of at least 70 percent of Canadian
women who abuse drugs. Most women at
the Canadian conference felt that 80 to 90
percent are more accurate figures as many
cases of sexual abuse go unreported.
What are the best ways to help these
women break their cycle of addiction?
Many individual treatments were discussed, but the participants agreed that in
order to be effective, any approach must be
comprehensive. A group in Southwest
Ontario, The Women Being Well Project,
says that the approach must be positive,
but holistic. No treatment program is likely
to work unless the causes of the addiction,
as well as the addiction itself are treated.
Detoxification must include treatment of
past sexual abuse and must be tailored to
meet the individual needs of the women it
serves.
The problems associated with drug
abuse are particularly poignant for women
of color. Maggie Hodgson explains the toll
that alcoholism takes on families of color,
"It is easy to understand why the tolls of
alcoholism are so high when one examines
the degree of personal and collective
misery that are ours." Drug addiction
treatment centers which cater to white
women often cannot address the issues of
concern to women of color; consequently
the treatments are ineffective. Ms. Hodgson
explains what has been done to meet the
needs of women of color: "We have formed
our own program called Nechi (translation:
my soul touches yours). Between 60 and 80
percent of our participants are survivors of
sexual abuse."
Ms. Hodgson espouses a philosophy
of healing that all women would do well to
remember: "We reclaim our spiritual
center and we work in concentric circles
towards the family, our women friends, our
community, and towards political action."
Further Reading:
• "Tranquility Can Kill," by Linda Rauch
Peregal,
Healthsharing,
a
Canadian
Women's Health Quarterly, Winter 1982.
• "The Politics of Quitting Smoking," by
Patricia Rawson and Debbie Holmberg
Schwartz, Herizons, a Canadian women's
news magazine, December 1984.
Connexions 25 Winter 1987 23
Together
We
Switzerland/Nicaragua
(Excerpted from "Support through SelfHelp" in Women's World, an Isis International publication, no. 8, December 1985,
and "Internationale Kontakte des FFGZ"
in Clio, a West German feminist self-help
magazine, no. 26, March 1987.)
The Dispensaire des Femmes in
Geneva is an autonomous women's health
center set up in 1978. The sixteen women
of the Dispensaire work as a collective.
The aim of the center is to provide preventive health care and information and to
help women gain better control over their
own bodies and health. They do research
into and provide alternative treatment,
including
naturopathy,
acupuncture,
homeopathy, and nutrition. One of the
members of the collective, Rina Nissim,
has written a highly successful book on
natural healing in gynecology. On visits to
Nicaragua, Nissim established contacts
with various women's groups there.
Many women in Nicaragua are illinformed about their bodies and their fertility. A study conducted at the Berta Calderon maternity clinic in Managua showed
that 10% of the women who had an illegal
abortion died of the ensuing complications,
and that another 25% remained permanently sterile as a result of abortionrelated infections. Nicaraguan women are
working toward reform of the law that
declares abortion illegal, and they are trying to make information on contraception
and sexuality more readily available. They
asked the women from the Geneva Health
Collective to share their experience and
knowledge with Nicaraguan women.
The women from Switzerland and
Nicaragua decided to collaborate on a
health project. They traveled around the
country in a car equipped with informational material, specula, diaphragms, gel,
surgical utensils, gauze, etc. During the
summer of 1987, this "mobile women's
health center" visited various women's
groups in Nicaragua in order to acquaint
women with basic knowledge about health
and contraception and to support them in
their demand for self-help.
This movable project makes it possible to transmit knowledge from one selfhelp group to another in spite of limited
resources. Through the travel of one
woman equipped with the necessary
materials, many women can be reached.
24
Connexions 25 Winter 1987
Are
Piers Cavendish/Reflex
Mauritius
"Disease NO-Health-YES: A Medical Manual," is a booklet published by four
progressive Mauritian organizations: the
Bambous Health Project, the daily LAUT,
the Women's Liberation Movement, and
the literacy program "Education for Work"
in 1986. The literacy program, which compiled, printed and distributed the booklet,
also used it in their courses. The booklet,
written in Creole (which is spoken by 52
percent of the population), explains in an
accurate and accessible manner how local
diseases come about, how to to cure them,
and most importantly, how to prevent
them. It covers a range of illnesses including amoeba-related illness, appendicitis and
AIDS. With regard to the latter, the
manual stresses the fact that anvone, not
just male homosexuals, can be affected by
the disease.
The Bambous Health Project is a
cooperative founded in May 1975. An executive committee takes care of organizational tasks. The project employs a fulltime doctor and 350 families participate.
In 1978, a pharmacy with all essential
medicines was set up. In addition, a oneyear training course for health volunteers
was instituted. The course trains villagers
in basic knowledge of health and hygiene
in order to break the monopoly of the medical profession-once they go back to their
village they organize their fellow villagers
to eradicate various diseases. The courses
are taught in Creole. The syllabus
comprises functions of the body, first aid,
nutrition, occupational disease, women's
diseases, contraception, pregnancy, alternative care and preventive medicine. According to the manual, 25%-35% of all diseases
could be prevented. The Bambous Health
Project considers itself an alternative to
both the private medical establishment and
the National Health Service. Private medicine is prohibitively expensive, and statecontrolled health care is afflicted with
bureaucratic control, corruption and political favoritism.
Strong
Bangladesh
(Translated from "International Contacts
of the FFGZ" in Clio, a West German
feminist self-help magazine, no. 26, March
1987.)
In 1976, Rokeya Begum founded a
women's self-help project called "Self Reliance Development Society" in Netrakona,
Bangladesh for women from the nearby
slums. Over the course of seven years of
organizing and lobbying, Rokeya gained
the support of the better-off women in
Netrakona. She even received a government credit of $US 5000. With this money,
she built a small building to house the project and bought two sewing machines, a
knitting machine and an embroidery
machine. Seventy women found paid jobs
in the project. They manufactured clothes
and batiks, sisal wall hangings, bamboo
furniture, etc. Soon afterwards the project
was expanded. A day care center for children from the slums was set up-the children receive milk at the center once a
week. The center offers courses on healthrelated issues and contraception as well as
basic literacy programs. The demand has
been so high that the women can only work
for a few hours at a time; they have to
alternate and many women cannot even be
admitted.
The center has often been the target
of state control; it was shut down several
times for political reasons. In 1985, the
machines were confiscated because the
women refused to have their project turned
into a propaganda instrument of the
government. In 1986, the women had to
start again from scratch. Rokeya and other
women worked tirelessly on the reconstruction of the center. The women have started
to work there again, and they plan on setting up a small women's health center.
Monique Jacot/Dispensaire des Femmes/ISIS
Berlin
(Translated and excerpted from "Feministische Selbsthilfe und Gesundheitsarbeit im
Rahmen konservativer Sozialpolitik-Eine
Standortsbestimmung" in Clio, West German feminist self-help magazine, no. 23,
May 1985.)
The Feminist Women's Health Collective was founded in 1977. The Collective was organized as a politically
motivated self-help group. Our purpose is
to make sure that women become fully
acquainted with their bodies and become
responsible for their health. We encourage
women to work with other women to set
standards of health and sexuality. We also
want to reinforce the awareness that health
and disease are intimately related to the
overall living condition of women.
We work to provide this service for
little or no pay. We publicly demand that
women should not have to do any unpaid
labor, but have been unable to realize this
goal for ourselves. As an autonomous project, we depend on income generated by
the Collective and on donations. Most of
us must have other income in order to pay
our bills. But we do find that working to
better women's lives is very satisfying and
meaningful work.
Our services at the health collective
help to balance the deficits of the statecontrolled health system. We have always
considered our work not only a reaction to
existing shortcomings or a correction of
gaps in the state-controlled health system,
but also a necessity in the movement
toward control by women of their own
bodies. We did not expect financial assistance from the government, as we believed
that self-determination for women could
only take place in an autonomous group.
We deliberately disassociated ourselves
from traditional patriarchal institutions
such as the government health care system.
Ironically, that same system has recently
begun to praise the women's self-help
movement. The government intends to
reduce state-sponsored care to a supplemental resource and eventually plans to
abolish it altogether.
The government's new alliance with
the alternative health movement is highly
suspicious.
Conservative
government
officials have finally assessed the economic
value of the alternative projects-they conceive of the services as an effective means
to save government money. During the
recent economic crisis, many women were
laid off. The unemployment rate among
women doubled from the years 1981 to
1983. Instead of having paid jobs, women
were expected to perform some form of
social work. Ultimately, this means that the
government is unjustly making money off
of women's unpaid labor.
The budget for social services has
been cut and self-help groups are suddenly
deemed important in supplementing state
services. How does this translate into daily
politics? While the state-run hospitals in
Berlin cut two thousand jobs (which saves
the state 100 million DM), state agencies
encouraged private non-profit organizations
to create 467 jobs for social workers (which
costs the state 5.2 million). The pseudoprogressive rhetoric surrounding these drastic measures suggests that social services
are being qualitatively improved, whereas
in actual fact the measures represent
regressive social politics implemented
mainly at the expense of women.
In June 1982, women's and alternative projects were supposed to receive 10
million DM. In the fiscal year 1983, this
amount had shrunk to 7.5 million, and was
further decreased in 1984 to 6.5 million.
Only half of these monies were directly
allocated to various projects; the other half
mysteriously disappeared into the state
bureaucracy. Moreover, the intention was
by no means to gradually provide salaries
to more self-help workers, but to allocate
just enough money for a part-time or a
full-time position; one of the main functions of the recipient of that job was to
mobilize and organize volunteers. The
privatization of public services is presented
as a solution to social problems, but in
essence, current social politics will result in
the exploitation of self-help health workers.
Further Reading:
• CLIO, a West German feminist self-help
magazine, FFGZ, Bambergerstr. 51, 1000
Berlin 30 (West).
Natural Healing in
Gynecology, A Manual for Women, by
Rina Nissim, R outledge and Kegan Paul,
London 1986.
Clio
c:IOC: DC1011rr1' ZCIIS(nrlll
zur SCIDllnllFC:
26
WOMEN IN THE BAY AREA
We need more volunteers to help with upcoming issues. If you are interested in working on
our project, have language, editing, layout or fundraising skills, we'd like to hear from you.
See our address on the inside back cover.
Connexions 25 Winter 1987
25
Shorts
Canada
(From the proceedings of the Coalition of
Provincial
Organizations
of
the
Handicapped's Workshop on Disabled
Women's
Issues;
edited
by
April
D' Aublin/Research Analyst; March 1987,
Reproductive Rights Workshop by Maria
Barile.)
I want to make it clear that when I
talk about "choice," I am talking about
choice in all areas-the choice to have children, to have an abortion, or to adopt children.
The reproductive rights of women
involve four areas. All women must be free
to prevent and end unwanted pregnancies
regardless of their economic means.
"Reproductive rights" also implies that
women should be able to choose if, when
and how to have children. This means that
no woman should be forced into abortion
or sterilization, or to risk infertility due to
dangerous birth control methods such as
Depo Provera and the Dalkon Shield.
Disabled women in particular are
discriminated against with respect to reproductive rights. Many people believe that
disabled women are psychologically incapable of conceiving and bearing childrenthat disabled women must decide not to
have children. From a very early age,
women are made to feel that they have a
responsibility to produce healthy childrena disabled child is seen as a woman's
failure. Because some disabled women have
a greater chance of having a disabled child,
disabled women are often coerced into
unwanted abortion and sterilization. In
addition, disabled women are often sterilized without first having been given the
facts about the procedures involved.
If a disabled woman chooses to have
children, then the questions arise: Who will
care for the infant? Who will pay for extra
help or specialized technical aids? When it
comes down to it, it is a socio-economic
question that our able-bodied sisters do not
need to consider. A disabled women is
always made to feel that the choice is not
hers and her partner's but that of the state.
On the question of abortion, disabled
women share with every other woman the
concern for safe and economical abortion.
Most often disabled women, unlike ablebodied women, are encouraged to have
abortions when they become pregnant,
even if they are pregnant by choice. The
Office of the Handicapped does not have
any plan for dealing with childbirth or children. Disabled women are also able to get
an abortion more easily than most other
women. Now I don't mean to sound prolife, but our private choice is limited
because we are disabled.
There is another problem that comes
with reproductive "choice". Through
amniocentesis, women are now able to find
out if their fetus is disabled. Women can
then abort the fetus if they choose. It is a
responsibility of those of us who have lived
as disabled people to make sure that
women find out that it is O.K. to live as a
disabled person, and that we have good
lives regardless of our disabilities.
Switzerland
'.'j
-,,,
"c:,
!:=
.~
(Submitted by Elizabeth Ferris, World
Council of Churches, Geneva, Switzerland,
November 1987.)
c::i
~
26 Connexions 25 Winter 1987
~
~
:i:;
§
"I had the feeling that I was dirtying
the boat by my mere presence. The others
left me more room-either out of pity or
because I was 'dirtier' than they were. I
was glad if they avoided looking at me."
These words, spoken by a Vietnamese
refugee about her rape by pirates, convey
some of the pain that many women
refugees face during flight. Although this
young woman received medical care and
counseling when she arrived in Pulau
Budong, Malaysia, the physical and emotional consequences will last for many
years. The many victims of pirate attacks
are but one example of the violence that
many refugee women face during their
flight to safety. The violence takes many
forms: from abuse at European airports to
forced prostitution along the Mexican
border to sexual exploitation by border
guards in Djibouti. The scars of violence
run deep, leading to physical and emotional trauma-trauma compounded by the
experiences of exile.
It is difficult to generalize about the
world's 15 million refugees. But, most
refugees around the globe are women and
girls and they do face particular health
problems. Like all refugees, women often
cross borders in a state of exhaustion.
Some have experienced pursuit, others
have walked for days with little food or
water. For refugees arriving in camps or
settlements, often times there are inadequate water supplies and poor sanitation
facilities. These conditions are conducive
to breeding many diseases-refugees are
particularly susceptible because of their
poor physical state upon arrival. Women
often experience malnutrition especially
when they are pregnant or breast-feeding.
Also, if the food supply is limited, mothers
may neglect their own needs in order to
feed their children first.
But along with the physical conditions, other factors, less understood by
relief officials, influence the health of
refugee women. Women are the traditional
guardians of culture and are often the ones
trusted with keeping families together.
Because of this, refugee women feel
disoriented by having their culture
uprooted and families separated-they are
unsure of their role in the new environment.
Although the vast majority of the
world's 15 million refugees are women,
health services are not set up to meet their
netids in many countries. As a woman
working with Ethiopian refugees explains,
"because the women are responsible for
collecting fuel and water and for taking the
children to health care and feeding programs, they are the last to receive health
care. When the out-patient department was
finally set up, men made up 67 percent of
the patients. The women did not have the
time." For Moslem refugees, cultural factors also limit women's access to health
care. In Pakistan, for example, most of the
2-1/2 million Afghan refugees are women
and girls. Yet, they can receive medical
treatment only from women doctors, who
are in woefully short supply. This contributes to further malnutrition and disease.
Refugee women not only have serious health needs, but also have an important role to play in preventing disease, promoting nutrition, and in educating the
community about the importance of safe
water. Their knowledge and experience in
traditional medicine is a resource to be
used by the community. Refugee women
must continue to demand a greater role in
making the decisions that affect their
health and the health of their children.
Malaysia
(From Women in Action, an Isis International publication, Supp. n.6, December
1986.)
The Malaysia-based Third World
Network has issued an urgent call for
action to pressure the World Health Organization to reverse a policy decision on
breastmilk substitutes for newborn children. The policy threatens to undo some of
the hard-won gains of the decade-long,
worldwide campaign by women's and consumer advocates groups to limit multinational corporations' promotion and marketing of breastmilk substitutes, particularly in
developing countries.
The policy came as a result of a
request by many countries for guidelines
clarifying the intent of the International
Code on the Marketing of Breastmilk Substitutes, a model code for national legislation adopted by the World Health Organization in 1981 for limiting the marketing
and promotion of bottled milk products.
Though grassroots groups consider the code
a crucial victory in the struggle to protect
breastfeeding from unfair commercial competition, one criticism they have raised all
along is that the code still leaves sizable
loopholes for infant formula companies.
pients of free or subsidized supplies of
breastmilk substitutes. (One gaping loophole in the Code has permitted infant formula companies to continue giving large
amounts of free milk supplies to hospitals
and clinics.) However, this crucial provision was omitted from the final guidelines
published by the World Health Organization in May 1986.' Anonymous sources
inside WHO admitted to the daily newspaper International Herald Tribune that the
provision was omitted because of pressure
from the United States and baby food
manufacturers.
The development represents a blow
to the pro-breastmilk movement after so
many
years
of fighting
for
the
WHO/UNICEF International Code and
launching a highly successful campaign
against the Nestle corporation, one of the
major infant formula companies.
The Third World Network asks individuals and groups to write letters expressing their concern over the matter and urging the agencies to reinstate the provision
regarding free supplies.
Contact:
• Third World Network,
87 Cantonment Road,
Penang, Malaysia
New Zealand
(From Women in . Action, an Isis International publication, Supp. no. 6, December
1986.)
lfiEles
-artifici&I iff\i tat\On
BKBY Ft>OD
Partly for this reason, health and policy experts from eight countries met with
WHO and UNICEF staff in December
1985 to draft guidelines for implementing
the code. One of the most important provisions they agreed upon was that maternity
wards and hospitals should not be the reci-
The New Zealand Women's Health
Network is a national network of feminists
concerned about health. The group, created
ten years ago, aims to provide a forum for
women, especially non-health professionals,
to discuss and educate one another on
health problems and develop responses to
local and national health policies. The network defines health in the broadest sense,
encompassing social and economic issues
such as alcohol abuse, disabled women's
sex problems, lesbian motherhood, incest,
industrial health, and patient's rights.
The group carries out a series of regular activities, including publishing a
bimonthly newsletter, organizing occasional
conferences and workshops, and distributing resources such as a friendly and accessible booklet Coping with Menstruation:
Information for Disabled Women. Besides
dealing with the concerns of disabled
women, the group's publications and programs also focus on the health situation
and needs of the islands' indigenous Maori
women. Finally, the network puts New
Zealand women's health groups in touch
with women's health groups in other countries.
Contact:
• New Zealand Women's Health Network,
P.O. Box 2312,
Tauranga, New Zealand.
Connexions 25 Winter 1987 27
(cont. from p. 11)
HELAINE VICTORIA PRESS
little tolerance for abnormalities, diseases and disabilities. I think
the motivation behind this intolerance is related to the desire to
keep a " superior" gene pool in German society-a desire which
has a historical base in eugenic actions taken by the Nazis.
In fact, research indicates that many of the women who
were sterilized by Nazi orders led lives that today we would call
" feminist." In the special Nazi courts that dealt with forced
sterilization, these feminist women were labeled "socially disabled" and therefore candidates for sterilization. It is very frightening to see that involuntary sterilization of women continues in
West Germany. But now the issue is being debated with a historical perspective that I hope will motivate people to eliminate the
attack on disabled women's reproductive rights. □
A SMALL FEMINIST
PRESS SPECIALIZING IN
WOMEN 'S HISTORY
POSTCARDS FOR OVER
14 YEARS.
~~
Important & dynamic
photos on the front &
biographical capti o ns
on the back .
Contact:
• Theresia Degener
2318 Parker #A
Berkeley, CA 94704
or
Prozessionsweg 8
4417 Altenberge, Federal
Republic of Germany
• Anneliese Mayer
C/O AG SPAK
KISTLERSTR. l
8000 Munchen 90
Federal Republic of
Germany
• Judy Heumann
World Institute of Disability
l 720 Oregon Street #4
Berkeley, CA 94703
Further Reading:
• With the Power of Each Breath, A Disabled Women's Anthology, Edited by Susan E. Browne, Debra Connors, and Nanci
Stern, Cleis Press, Pittsburg, PA, 1985.
• Geschlecht: Behindert, Besondered Merkmal, Frau, (A book by
and about disabled women), C. Ewinkel, G. Hermes, and others
(eds.), AG SPAK M68, Munchen, 1985.
• Kruppel-Tribunal, Menschenrechtsverletzungen im Sozialstaat,
(A book about violations of disabled peoples rights), Edited by
Susanne V Daniels, Theresia Degener, Andreas Jurgens, Frajo
Krick, Peter Mand, Anneliese Meyer, Birgit Rothenberg, Gusti
Steiner, and Oliver Tolmein, AG SPAK, Munchen, 1983.
• "Das Bose Erbe," Emma, a West German feminist monthly,
November, 1984.
• "Die sollen-und die anderson durfen nicht," Emma, a West
German feminist monthly, August, 1985.
Special focus on
Black & Latin
American women,
U.S . Latinas , labor
history & other
topical material.
Madam C.J Walker, Black
millionaire & philanthropist
Send $1 . for catalog & 2 sample cards .
Helaine Victoria Press , Dept. Cx .,
411 E. 4th St. Bloomin ton , IN 47401
Qay
CWomett
For a change in your life we invite you to
,
try: The Wishing Well Magazine. Features
hundreds of current members' self-descriptions (by
Code #), letters, opinions, valuable resources, reviews,
and much more. Introductory copy $5.00 ppd. (mailed
discreetly first class). Confidential , supportive, dignified,
sensitive, prompt. Beautiful, tender, loving alternative
to "The Well of Loneliness." Fully personal, noncomputerized. Reliable reputation. Established 1974.
The pioneer of them all! Free information. Gay
women are writing and meeting EVERYWHERE
through:
en. r1 1 1 ,. r1 1 1_11n P.O. Box G
une ~wisnlttg ~w~\:'. Santee, CA 92071
I
BIG MOUNTAIN Help maintain s3cred lands at
Big Mountain . Inspiring new fullcolor poster with artwork by
Andrea Kay Smith. 25x32 . By
mail, $22 .50. Send $ 1 for fall '87
full-color catal og of posters,
cards and th e Carry It On Peace
Cal endar Wh olesale welcome.
VISA/ MC.
Pl4 580
SYRACUSE CULTURAL WORKERS, Box 6367, Syracuse, NY 13217 (315) 474-1132
28
Connexions 25 Winter 1987
rr- ~
~
Thank you so much! I think Connexions is wonderful-it helps to transcend
boundaries and barriers .. .! wish only the
best for the collective.
Sincerely,
Joanne M. Ursino
Ottawa, Ontario
Canada
Greetings! I received my very first
issue of Connexions on women in the
visual arts and needless to say, I've enjoyed
it tremendously! I am proud to be on the
Connexions mailing list. "Nakedness:
Movement and Confrontation" made me
realize that our bodies are such wonderful
works of art. Too bad one can't be seen
without all the negative additives.
The article on "Shared Moments
with Working Children" was great too
-very enlightening. It's a sad affair how little children are exploited.
The article "Agents of Change" was
like a breath of fresh air! Beautiful. This
article holds my ideal concept of progressive change. I personally feel that it would
be nearly impossible to convince many
men of the importance of women in our
society, but we can teach our sons and
daughters that men and women are of
equal worth. Perhaps if the same approach
that "Agents of Change" demonstrates is
utilized in our country, we might see progressive change happen in our lifetime. Oh
how I wish the feminist movement success
and pray for an awakening in the minds of
men.
In Solidarity,
Comrade Charles Logan
Jackson, Michigan
Gabriel's
apartments & guest rooms
for women & their friends
(617) 487-3232
104 Bradford Street
Provincetown, MA 02657
,,;:-__,_. ~--:-i \ "~':_:..i"~
Her eyes are miniature globes, in them there
is a country, one she visits while she
rocks and hopes the country disappears.
She sits on the cold shore, tugging her hair,
watching the clouds strain rain over the sea;
her eyes are miniature globes, in them there
is a country. That one she tried to tear
out of an eye. All day she watches, sleeps,
rocks and hopes the country disappears.
With )1er hands she covers her eye, the glare
of the sun deranges her diminutive dreams.
Her eyes are miniature globes, in them there
behind the rainstorms, into the blue air
yet it doesn't. She sits, waiting for weeks.
Her eyes are miniature globes in them thererocks and hopes; the country disappears.
J
ya -;-c .
•
Politics and Teaching
Do Mix
Feminist Teacher, a magazine
for teachers of all grade levels, in
traditional and nontraditional settings
• articles
• interviews
• bibliographies
• book reviews
• news and more
Feminist Teacher
Three times per year.
Ballantine 442
$12 U.S., $15 Canada (US Funds)
Indiana University
$16 outside North America
Bloomington, IN 47405
Name _______________________
Address _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ __
Teaching interests, institutional affiliation:
Woman Waiting
are castles with rooms, but they are bare
Staring at the dark stones, she violently
rocks and hopes the country disappears
Gabriel Brooke, Innkeeper
Open Year Round
Cable TV & Coffee
Hot Tub & Sun Deck
In the Center of Town
(Submitted By Marisella Veiga, Santurce,
Puerto Rico)
ERRATA for VISUAL ARTS# 24
on p. 3-Doris Lotch should read Doris
Lotsch
on p. 25-par. 1: April 27, 1987 should read
April 27, 1986
on p. 26-GSMG+K should read GSMB&K
Gesellschaft Schweizer Malerinnen, Bildhauerinnen
&
Kunstgewerblerinnen
(member IAWA)
on p. 27-Centre Audiovisuel, Simone de
Beauvoir should read Centre Audiovisuel
Simone de Beauvoir
on p. 27-Christa Biedermann, artist should
read Christa Biedermann and Krista Beinstein, artists
on p. 27-Rahnuma Ahmed, artist should
read Rahnuma Ahmed, Nari Shongoti,
Dilara Begum Jolly (CONTRIBUTORS),
Center for Social Studies, Arts B1 Dhaka
University, Dhaka, Bangladesh
on p. 27-Jin Sook Kim, artist should read
Jin-suk Kim and In Sook Kim, artists
on p. 27-Duloe Maria Lopez Vega should
read Dulce Maria Lopez Vega
on the back cover, the caption and credit
should read "Witch" from the series
"Witch-Pictures," Krista Beinstein, camera
and Christa Biedermann, in front of camera
We apologize for any inconvenience our
inconsistencies may have caused.
Connexions 25 Winter 1987
29
Health Resources for Women
••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••••
Argentina
Mabel Bianco, Coordinator of the Women, Health, and Development Program, Defensa l 20-4piso, of. 4080, ( 1345) Buenos
Aires, Argentina
Australia
Adelaide Women's Community Health Centre, 64 Pennington
Terrace, North Adelaide 5006, Australia
Leichhardt Women's Community Health Centre, 164 Flood
Street, Leichhardt, New South Wales, 2040, Australia
Liverpool Women's Health Centre, 273 George Street, Liverpool,
Australia
Austria
Osterr AIDS Hilfe, Lenaug. 17, A-1080, Vienna, Austria.
Bangladesh
Consumers' Association of Bangladesh, 32012A West Dhanmandi
Road, No. 8A, Dhanmandi RIA, Dhaka, Bangladesh
Belgium
Aimer d Louvain la Neuve, Cour des 3 Fontaines 31, 1348
Louvain la Neuve, Belgium
Brazil
Centro Informar;do Mu/her, (contact for further listings of
women's health groups in Brazil), Caixa Postal 11.399, 05499
Sao Paulo, SP, Brazil
Dominican Republic
Colectivo Mujeres y Salud, Apartado 22248, Santo Domingo,
D.N., Dominican Republic
France
Groupe Pratique Sante, 15 Rue J.B. Say, 69001 Lyon, France
Hong Kong
Asian Community Health Action Network, Flat 2A, 144 Prince
Edward Road, Kowloon, Hong Kong
India
Women's Centre, (information about amniocentesis and other
women's health issues), 104B Sunrise Apts. Nehru Rd., Vakola,
Santa Cruz (East), Bombay 400 055, India
Voluntary Health Association of India, C-14 Community Centre,
Safdarjung Development Aera, New Delhi 110 016, India
Rural Women's Health Group, Rural Development Society, 15/1
Periya Melamaiyur, Vallam Post, Chingleput 603002, South
India
Ireland
Dublin Well Woman Centre 73 Lower Leeson Street, Dublin 2,
Ireland
Ulster Cancer Foundation, 40/42 Eglantine Avenue, Belfast BT9
6DX, Northern Ireland
Defend the Clinics Campaign, National Committee, 6 Crow
Street, Dublin 2, Ireland
Sexo Explicito, (a feminist publication often concerned with
health issues), Casa da Mulher: Rua Debret, 23/13 I 6 CEP 20030,
Rio de Janeiro, R.J ., Brazil
Coletivo Feministe Sexualidade e Saude (feminist health center),
Rue Baltezar Carrasco 89, Piuheiros, Sao Paulo, S.P. , Brazil
SOS Corpo, (feminist health organization), Rue do Hospicio
859/ l 4, Recife, P.R., Brazil.
r;_~
__
Canada
Women Health Sharing, 101 Niagara St., Suite 200 A, Toronto,
Ontario, Canada
Coalition of Provincial Organizations of the Handicapped, 926294 Portage Avenue, Winnipeg, Manitoba R3C 0B9, Canada
Coalition of Provincial Organizations of the Handicapped,
Women's Caucus 456 West Broadway, Vancouver, B.C., Canada
Centre de Sante des Femmes du Quartier, 16 Est Bd., St. Joseph,
Montreal, Canada
The Immigrant Women's Centre: Mobile Health Clinic, 348 College Street, Toronto, Ontario, Canada MST IS4
Calgary Women's Health Collective, 2340 I Ave. N.W. Calgary,
AB T2N 0B6 Canada
Dis-Abled Women's Network, 122 Galt Avenue, Toronto,
Ontario, M4M 2Z3, Canada
China
Institute of Chinese Medicine, Gynecological Research Department, Zhang Jingling, Hunan Province, People's Republic of
China
Colombia
Grupo de Ajude e Inforinacion, (AIDS Information), c/o Manuel
Antonio Velanda Move, Apdo. Aereo 25770, Bogota I, Colombia
Costa Rica
Centro Feminista de Informacion y Accion, Apdo. 5355 San Jose
I 000, Costa Rica
30
Connexions 25 Winter 1987
I
J;
1£·
-'
i
Marie Falksten
© ,
Vrouwengezondheidscentrum Katelijne (women's health center),
Walstraat 5, 4531 ED Terneuzen, Netherlands
Platform Vrouwen en AIDS (women's AIDS information centre),
Maliesingel 46, 3581 BM Utrecht, Netherlands
New Zealand
Hecate Women's Health Collective, P.O. Box 11-675, Wellington,
New Zealand
New Zealand Women's Health Network, C/O Sarah Calvert, P.O.
Box 2312 Tauranga, New Zealand
Nicaragua
Festasalud, Matagalpa, Nicaragua
Nigeria
Hannah Edemikpong, Women's Centre, (information on AIDS
and genital mutilation in Africa), Box 185, Eket, Cross River
State, Nigeria, W. Africa
Peru
Italy
Gruppo Feminista per la Salute Della Donna, Vicola San Francesco a Ripa 17, 00153 Rome, Italy
Japan
Soshiren, (Committee Against Revision of the Eugenic Protection
for Reproductive Freedom, C/O JOKI, Nakazawa Bldg. 3F, 23
Arakicho, Shinjuku, Tokyo, Japan
Women's Health Action Network of Japan, C/O Japanese
Women's Council, Products Bldg., 1-33-3 Hongo, Bunkyo-ku,
Tokyo, Japan
Sapporo Group to Stop the Retrogressive Revision of the Eugenic
Protection Law, C/O Hirahira, 2F, Nishi 5-chome, Kita 18-Jo,
Kita-Ku, Sapporo City, Japan
Women's Health Center, 2-6-2 Tamatsukuri, Higashi-Ku, Osaka,
Japan
Feminist Therapy, 93-3-24 Okanouemachi, Toyonaka City,
Osaka Prefecture, Japan
Women's Body's Network "Maimai," C/O Hayakawa, 1-44
Yasakacho, Nishi-Ku, Nagoya City, Japan
Feminist Therapy, "Nakama," Rm. 302 Kihara Bldg., 17
Saneicho, Shinjuku-ku, Tokyo, Japan
Asian Women's Association,
14-10-211 Sakuragaokacho,
Shibuya-ku, Tokyo, Japan
Kenya
National Council of Women, P.O. Box 43741, Nairobi, Kenya
Breast Feeding Information Group, P.O. Box 59436 Nairobi,
Kenya
Centro de Documentacion Sohre la Mujer, Av. Arenales 2626,
Lima 14, Peru
Puerto Rico
Taller Salud, Apartado 2172, Hato Rey Station, Hato Rey,
Puerto Rico, 92172
Philippines
Gabriela, Room 221, PCI Bank Bldg., Greenhills Commercial
Center, San Juan, Metro Manila, Philippines
South Africa
Critical Health,
Central
Printing
Unit/University
of
Witwatersrand, I Jan Smuts Avenue, Johannesburg, South Africa
South Pacific
Maternal and Child Health Department, Central Administration,
P.O. Box 149, Niue Island, South Pacific
Switzerland
World Council of Churches, Elizabeth Ferris, Refugee Service,
P.O. Box 66, 150 Route De Ferney 1211 Geneva 20, Switzerland
AIDS-Hilfe Schweiz, Postfach 1054, CH-8039, Zurich, Switzerland
Dispensaire des Femmes, 4 rue du Mole, 120 I Geneva, Switzerland
Fraungesundheitszentrum, Sulgeneckstralle 60, 3000 Bern,
Switzerland
Frauenambulatorium, Mattengasse 27, 8005 Zurich, Switzerland
Thailand
Women's Information Centre, I I 3/9 Charasanitwong Road 46,
Bangkok I 0700, Thailand
Malaysia
Health Action International, P.O. Box 1045, 10830 Penang,
Malaysia
Consumer's Association of Penang, (publishes information on
women's health issues), 87 Cantonment Road, 10250 Pulau,
Penang, Malaysia
Mauritius
Muvman Liberasyon Fam, 5 Rue Street, Therese, Curepipe,
Mauritius
Mexico
IXQUIC, (published a pamphlet on women and health in Guatemala, May 1987), Apartado Postal 27-008, C.P. 06760 Mexico,
D.F., Mexico
The Netherlands
Women's Global Network on Reproductive Rights, P.O. Box 4098,
Minahassastraat I, 1009 AB Amsterdam, Netherlands
Vrouwengezondheidscentrum Utrecht (women's health center),
Maliesingel 46, 3581 BM Utrecht, Netherlands
Vrouwengezondheidscentrum Amsterdam (women's
health
center), Obiplein 4, 1094 RB Amsterdam, Netherlands
Connexions 25 Winter 1987
31
United Kingdom
Women's Health Information Centre, 52-54 Featherstone St.,
London, ECIY 8RT, United Kingdom
The New Internationalist, (an English progressive monthly which
often includes articles on women's international health issues},
120-126 Lavender Avenue, Mitcham, Surrey CR4 3HP, United
Kingdom
International Contraception, Abortion, and Sterilization Campaign, 374 Grays Inn Road, London WCI, United Kingdom
United States
National Women's Health Network, 224 7th Street S.E., Washington, D.C. 20003
Women's Occupational Health Resource Center, Columbia
University, School of Public Health, 600 W. 168th Street, New
York, NY 10032
Feminist International Network of Resistance to Reproductive and
Genetic Engineering, P.O. Box 441216, West Somerville, Mass.
02144
Reproductive and Genetic Engineering: Journal of International
Feminist Analysis, Phyllis Hall, Vice President, Pergamon Press,
Maxwell House, Fairview Park, Elmsford, NY 10523
World Health Organization/Pan-American Health Organization,
525 23rd Street, N.W., Washington, D.C. 20037
Boston Women's Health Book Collective, Box 192, West Somerville, MA 02144
International Drinking Water Supply and Sanitation Decade,
Hilda Rwabazaire Paqui, United Nations Development Programme, Room DCl-1902, One UN Plaza, New York, NY 10017
Uruguay
Colectivo Maria Abella, Ma. Stagnaro de Munar 105, Barrio
Ciccsa, Paso Carrasco, Canelones Uruguay
West Germany
Pro Familia, a health counseling centre, Deutsche Gesellschaft fur
Sexualberatung u. Familienplanung, e.V. Beratungsstelle Schluterstr. 14, 2000 Hamburg 13 West Germany
Berliner AIDS-HILFE, (AIDS Information Center), Meinekestr.
12, 1000 Berlin (West) 15
Clio, Eine Periodische Zeitschrift zur Selbsthilfe, a feminist selfhelp magazine, Feministisches Frauen Gesundheitszentrum, e.V.,
Leignitzer Str. 5, I Berlin 36 (West)
Yugoslavia
Women, Society and Health Group, Student Cultural Centre, M.
Tita 58, I 1000 Beograd, Yugoslavia
Zambia
African National Congress, Women's Section P.O. Box 31791
Lusaka, Zambia
Zimbabwe
Women's Action Group, (Publishes information on women's
health issues}, Box 135 Harare, Zimbabwe
****************************************
"ba.J.man
rower ""'/
ll 111C(\!,llZil1C' of
feminism
spiritulllity
po/;th.,
An inspiring international quarterly publication
consisting of 96 pages of the highest quality women's
literary and artistic works. Lich issue explores a theme
central to an emerging planetary woman's consciousness in
a form,lt of interviews, articles, fiction, poetry, photograph y,
art, and profiles of womrn of power. Subscriptions S22. Single
issue $6 plus $1 postage.
"] 11 these times of
,\!,relit socilll chllll,\!,C',
if WC' l/TC' to
survive its ll species,
it is JJC'CC'SSllry
for women to
come into power
uncl for
feminist principles
to rebuild
the fournlntions
of world cultures. "
-woman of power
"Statement of Philosophy"
p.o. box 827, cambridge, ma., 02238
32
Connexions 25 Winter 1987
Classified Connexions
Classified Connexions!
Connexions classifieds reach over 15,000
readers for only 30 cents per word! All
ads must be prepaid. We reserve the right
to reject any ad and we cannot guarantee
placement of ad in any specific issue.
Deadlines are the first of February, May,
August and November.
Personals
Looking for a penpal? Selling a poster?
Organizing a conference? Then your
classified
belongs
here!
Connexions
classifieds reach over 15,000 women for
only 30 cents a word . Write Connexions,
4228 Telegraph Ave ., Oakland, CA 94609
for more information or send in your ad
with payment. Display ad rates also available.
Publications
Believe in Yourself Memo Pads boost
egos, give confidence. Try them . Send
$3.75 for 1, $17.50 for 5 to: Sol, Inc. (Attn :
Connie), Box 2111 , Hyatts, MD 20784.
Retailers query.
Lesbian of Color, 30, seeks to connect
with others age 25-35, who share interest
in art, farming , true appreciation for any
peoples of color; their culture respected.
Please write Marie Douglas, 200 Vassar
Drive , S.E., Albuquerque , NM 87106, USA.
Penpals
Instruction
Call for international penpals! Wishing to
exchange letters with other women. Let's
share our experiences. Sherry Hudson ,
3060 Marshall Avenue, #314, Cincinnati ,
OH 45220.
Goddesses, goats, and green witches
learn herbal medicine and spirit healing at
the Wise Woman Center with Seneca
leader Twylah Nitsch , shaman-singer Lisa
Thiel , herbalist Susun Weed , and others.
Free brochure of workshops, retreats, and
apprenticeships .
PO
Box
64CX,
Woodstock, NY 12498.
Lesbian Woman, 25 years old , seeking lesbian support. Contact: Ebere Chukwu, c/o
Dopa
Fashion,
4
Kenneth
Road ,
Awkunanaw, Enugu , Anambia
State,
Nigeria.
Travel
VISIT NICARAGUA: Intensive Spanish
courses, family living and community work
in Esteli . Scholarships available. Apply now
for 1988 sessions. NICA, PO Box 1409-CX,
Cambridge, MA 02238. 617-497-7142.
****************************************
Subscribe to Connexions
Order two issues and
get the third issue free!
Back issues: $3.00 + .75 postage per issue
□ One year, $12
Libraries and Institutions, $24
Canada and Mexico, US$ l 4
Overseas Airmail, US$20; Surface US$ l 4
□ Sustaining subscription, $25
(Donations are tax-deductible)
Make US checks (or international money
orders and travelers' checks) payable to
Peoples Translation Service and send to:
Connexions
4228 Telegraph Avenue
Oakland, California 94609
(415) 654-6725
Is this a gift?
From
Name
Address
City, State, Zip
Send me:
□ #24 Visual Arts
□ #23 Crisis and Transition
□ #22 Facets of Racism
□ #21 Education
□ #20 Marriage
□ #19 Women's Movements
□ #17/18 Forum '85/Nairobi
($6/double issue)
D #16 Media
□ # 15 Changing Technology
□ #14 Women Inside & Out
□ #13 Women's Words
□ # 12 Prostitution
□ #11 Women & Militarism (photocopy)
□ # l O Global Lesbianism II
□ # 9 Outrageous Women
□ # 8 Culture Clash
□ # 7 Young and Old Women
□ # 6 Environment-From the Ground Up
□ # 5 Women in Eastern Europe
□ # 4 Creativity (photocopy)
□ # 3 Global Lesbianism I (photocopy)
□ # 2 In Search of Work and Refuge:
Migrant and Refugee Women (photocopy)
□ # l Women Organizing Against Violence
(photocopy)
(Issues 1, 2, 3, 4, and 11 are only available
as photocopies)
Peoples Translation Service
Connexions
4228 Telegraph Avenue
Oakland, CA 94609
(415) 654-6725
$3.00
Non-Profit Organizatior
U.S. Postage Paid
Berkeley, CA
Permit No. 148
- Temporal Coverage
- 1980-1989
- Media
-
 Connexions_1987.pdf
Connexions_1987.pdf
- Hierarchies
-
Herland Archive
- All Resources (Private)
- Themes
- LGBTQ+ (482 items)
- Feminism (40 items)
- Faith and Religion (51 items)
- Activism and Advocacy (69 items)
- HIV/AIDS (25 items)
- Education (18 items)
- Literature (20 items)
- Art (16 items)
- Themes
- All Resources (Private)