
MedicalAlert.pdf
- Title
- MedicalAlert.pdf
- extracted text
-
DICAL
ERf
this issue sponsored by
Philip Morris Companies Inc. and
Ross Products Division of Abbott Laboratories
ISSUE ONE 1998
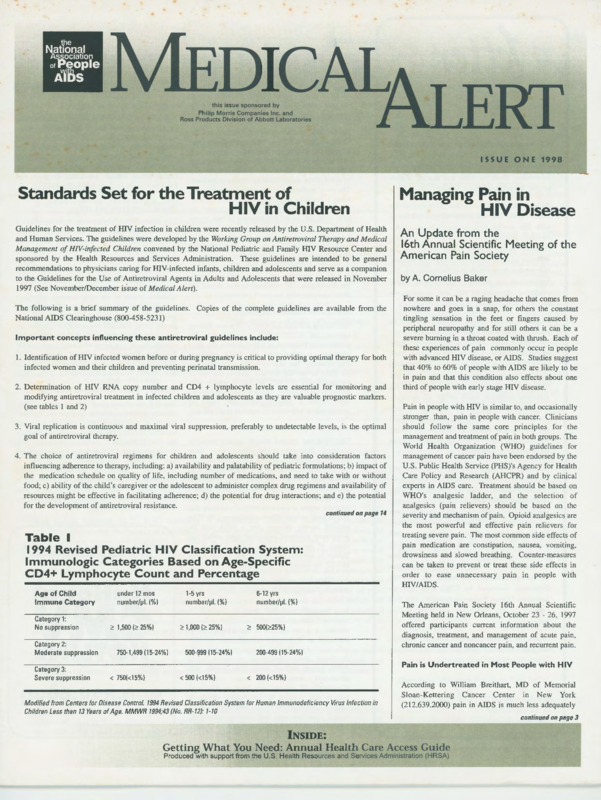
Standards Set for the Treatment of
HIV in Children
Guidelines for the treatment of HIV infection in children were recently released by the U.S. Department of Health
and Human Services. The guidelines were developed by the Working Group on Antiretroviral Therapy and Medical
Management of HIV-infected Children convened by the National Pediatric and Family HIV Resource Center and
sponsored by the Health Resources and Services Administration. These guidelines are intended to be general
recommendations to physicians caring for HIV-infected infants, children and adolescents and serve as a companion
to the Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents that were released in November
1997 (See November/December is.sue of Medical Alert).
The following is a brief summary of the guidelines. Copies of the complete guidelines are available from the
National AIDS Clearinghouse (800-458-5231)
Important concepts influencing these antiretroviral guidelines include:
1. Identification of HIV infected women before or during pregnancy is critical to providing optimal therapy for both
infected women and their children and preventing perinatal transmission.
2. Determination of HIV RNA copy number and CD4 + lymphocyte levels are essential for monitoring and
modifying antiretroviral treatment in infected children and adolescents as they are valuable prognostic markers.
(see tables I and 2)
3. Viral replication is continuous and maximal viral suppression, preferably to undetectable levels, is the optimal
goal of antiretroviral therapy.
4. The choice of antiretroviral regimens for children and adolescents should take into consideration factors
influencing adherence to therapy, including: a) availability and palatability of pediatric formulations; b) impact of
the medication schedule on quality of life, including number of medications, and need to take with or without
food; c) ability of the child's caregiver or the adolescent to administer complex drug regimens and availability of
resources might be effective in facilitating adherence; d) the potential for drug interactions; and e) the potential
for the development of antiretroviral resistance.
continued on page 14
Table I
1994 Revised Pediatric HIV Classification System:
Immunologic Categories Based on Age-Specific
CD4+ Lymphocyte Count and Percentage
Managing Pain in
HIV Disease
An Update from the
16th Annual Scientific Meeting of the
American Pain Society
by A. Cornelius Baker
For some it can be a raging headache that comes from
nowhere and goes in a snap, for others the constant
tingling sensation in the feet or fingers caused by
peripheral neuropathy and for still others it can be a
severe burning in a throat coated with thrush. Each of
these experiences of pain commonly occur in people
with advanced HIV disease, or AIDS. Studies suggest
that 40% to 60% of people with AIDS are likely to be
in pain and that this condition also effects about one
third of people with early stage HIV disease.
Pain in people with HIV is similar to, and occasionally
stronger than, pain in people with cancer. Clinicians
should follow the same core principles for the
management and treatment of pain in both groups. The
World Health Organization (WHO) guidelines for
management of cancer pain have been endorsed by the
U.S. Public Health Service (PHS)'s Agency for Health
Care Policy and Research (AHCPR) and by clinical
experts in AIDS care. Treatment should be based on
WHO's analgesic ladder, and the selection of
analgesics (pain relievers) should be based on the
severity and mechanism of pain. Opioid analgesics are
the most powerful and effective pain relievers for
treating severe pain. The most common side effects of
pain medication are constipation, nausea, vomiting,
drowsiness and slowed breathing. Counter-measures
can be taken to prevent or treat these side effects in
order to ease unnecessary pain in people with
HIV/AIDS.
Age of Child
Immune Category
Category 1:
No suppression
Category 2:
Moderate suppression
Category 3:
Severe suppression
under 12 mos
number/µL (%)
<! 1,500 (<! 25%)
1-5 yrs
6-12 yrs
number/µL (%)
number/µL (%)
<! 1,000 (<! 25%)
750-1,499 (15-24%)
500-999 (15-24%)
<! 500(<!25%)
The American Pain Society 16th Annual Scientific
Meeting held in New Orleans, October 23 - 26, 1997
offered participants current information about the
diagnosis, treatment, and management of acute pain,
chronic cancer and noncancer pain, and recurrent pain.
200-499 (15-24%)
Pain is Undertreated in Most People with HIV
< 750(<15%)
< 500 (<15%)
< 200 (<15%)
Modified from Centers for Disease Control. 1994 Revised Classification System for Human Immunodeficiency Virus Infection in
Children Less than 13 Years of Age. MMWR 1994;43 (No. RR-12): 1- 10
According to William Breithart, MD of Memorial
Sloan-Kettering Cancer Center in New York
(212.639.2000) pain in AIDS is much less adequately
INSIDE:
Getting What You Need: Annual Health Care Access Guide
Produced with support from the U.S. Health Resources and Services Administration (HRSA)
continued on page 3
ON the PULSE...
NIH Study on Mouth Sores
To the Reader:
NAPWA was founded 15 years ago with the belief
that people with AIDS would survive this
epidemic by equipping themselves with
information about the virus and sharing it with
others. We still hold this to be true.
Since 1992, Medical Alert has been one of the
tools NAPWA has used to provide you and others
with life saving information. From reader
responses and the number of request we get daily
from new people wanting to join the mailing list
we know its value to you. AIDS, or HIV disease,
has changed dramatically over the last year and it
has evolved into an even more complex health
condition. Because of this, our strategies are
changing to meet new challenges.
The National Institute of Dental Research and the
Clinical Center at NIH are looking for patients age
18 and older to take part in a study of a promising
new treatment for mouth sores associated with
HIV and AIDS. Those who qualify receive care
by some of the nation's leading experts in the field.
The study medication, a gel applied directly to the
sores, is provided at no cost. Participants can stay
on their regular course of medical treatment for
HIV or AIDS while participating in this study.
People or their doctors can contact NIH's Patient
recruitment and Referral Center for more
information: (Interested deaf or hard-of-hearing
callers should use their state relay services to
contact these telephone numbers) at 800.4 I 1.1222
or E-Mail: prrc@nih.gov. Patients living outside
the Washington, DC metropolitan area should ask
about compensation for travel expenses.
New Cytovene Capsule on the Market
Beginning with this issue, Medical Alert will be
published four times a year on a quarterly basis.
We believe this publication schedule better
reflects the flow of new scientific information and
medical advances. Our focus will also expand
slightly to provide more information on health
care access and quality of care, including working
with your physician, AIDS service organization,
and managed care provider to advocate for your
needs. Our Education staff will continue to assist
you in finding up-to-date information and linking
you to other national and local organizations
meeting your special needs.
NAPWA also takes this opportunity to welcome
Charles Nelson, our new Associate Director for
Health Education. Charles, a graduate in biology
from Morehouse College, is an African-American
gay man living with HIV who has long been
involved in treatment education and advocacy.
He has also been a member of the National Task
Force on AIDS Drug Development, convened by
the U.S. Department of Health and Human
Services and the Working Group on Guidelines
for the Prevention of AIDS related Opportunistic
Infections, convened by CDC, NIH and the
Infectious Disease Society of America. We look
forward to his leadership as editor of this
publication.
Thank you for your continued support. Together,
we will continue to learn and do what we must
to survive.
A. Cornelius Baker
Executive Director
2
Hoffmann-La Roche has introduced a new 500 ~g
capsule of CYTOVENE (ganciclovir) for
maintenance treatment of CMV retinitis, the most
common manifestation of CMV disease.
The company has also received approval from
the FDA to market the new capsule for use in
the prevention of CMV disease in people with
advanced HIV (AIDS). The new Cytovene capsule
will reduce a person's daily pill count of
ganciclovir in half-from 12 capsules to six per day.
Drug to Treat Crypto on Fast Track
The FDA has granted priority review status to
Unimed Pharmaceuticals, Inc. new drug
application (NDA) to market NTZ (nitazoxanide)
for the treatment of cyrptosporidial diarrhea in
people with HIV disease. This NDA is the first
application for treatment of the diarrhea associated
with cyrptosporidiosis. In immunocompromised
patients, crypto is a serious medical condition that
can be fatal without effective treatment. An FDA
priority review ensures that a NDA will be
completely reviewed and acted upon within six
month of receipt. Unimed holds an exclusive
license to develop and market oral dosage forms
of NTZ for human use in the U.S.
Regain Strength and Restore EnergyAnabolic Treatment for Anemia
In a recently published study by the CDC's
National Center for HIV, STD, and TB Prevention,
anemia, or a low number of red blood cells, is
indicated as a frequent complication of HIV
infection. According to the study, people who
developed anemia but never recovered had a
170% greater risk of death than people who
developed anemia but later recovered.
Chronically ill patients now have an additional
tool to help combat the debilitating effects of
anemia. Anadrol®-50 (oxymetholone) -- 50 mg
tablets -- is the only oral anabolic-androgenic
hormone indicated for the treatment of anemia.
National Association of People with AIDS
Anadrol®-50 helps people suffering from anemia
by stimulating red blood cell production by
enhancing the release of the body's own
erythropoietin, as well as directly signaling the
stem cells within the bone marrow to produce red
blood cells. Unimed Pharmaceuticals, Inc. has
established a Patient Assistance Program and
Reimbursement Hotline: 1-800-256-8918.
Drug Shown to Reduce Shedding of Herpes
Virus in People Living with HIV
The University of Minnesota recently released
results from a study led by Dr. Timothy Schaker
showing that Famciclovir (Famvir.., SmithK.Iine
Beecham Consumer Healthcare) when taken daily
significantly reduces asymptomatic shedding, the
time when the herpes virus is contagious but there
are no signs or symptoms, in HIV-infected patients
with genital herpes. Herpes simplex virus
infection is one of the most common infections
among people living with HIV. This study is
important because genital herpes outbreaks in
people living with HIV occur more frequently; are
especially severe; and can lead to life-threatening
complications. For more information, contact Dr.
Timothy Schacker, Assistant Professor of
Medicine at the University of Minnesota, at 1-612624-9955, or call Clara Morris at 1-212-598-2807.
Crixivan® Receives Full Approval by the FDA
The U.S. Food and Drug Administration (FDA)
recently granted traditional approval to Crixivan ..,
Merck & Company's HIV protease inhibitor,
based on the results from two studies that confirm
the clinical benefits of combination therapy with
Crixivan reduces AIDS-defining illnesses or death
and produces prolonged suppression of
HIV/RNA. Merck has developed, with the
American Dietetic Association, a list of foods,
light meals or snacks that can be taken with
Crixivan. For more information visit Merck's new
website www.crixivan.com.
NAPWA is committed to your survival.
For 24 hour confidential toll-free
information on CMV call the
National
CMV
HOTLINE
800·838-9990
(
Managing Pain
cantmued from page 1
treated than cancer pain. Recent studies cited by Dr. Breithart, during his keynote address, suggest that "only
6% of AIDS patients with severe pain are prescribed a strong opioid like morphine, despite the fact that the
WHO Analgesic Ladder suggests that clinicians consider using strong opioids in all patients with severe pain."
Using the Pain Management Index as a measure of adequacy of analgesic therapy, only 15% of AIDS patients
with pain receive adequate analgesic therapy, compared to almost 60% of cancer pain patients. Dr. Breithart
has also found that women with AIDS-related pain are twice as likely to be undertreated than men. People
with less formal education and those who contracted HIV through injection drug use are also more
undertreated for pain.
The following chart provides information on opioid analgesics:
Opioid Analgesics
Drug
Length of Effectiveness
Other Information
Morphine
Intravenous or intramuscular-2 to 3 hours
By mouth-3 to 4 hours
Sustained release~ to 12 hours
Starts to work quickly. Oral form can be very
effective for cancer pain
Codeine
By mouth-3 to 4 hours
Less potent than morphine. Sometimes taken with
aspirin or acetaminophen
Meperidine
Intravenous or intramuscular-3 hours
By mouth_:_not very effective
Can cause seizures, tremors, and muscle spasms
Methadone
By mouth-4 to 6 hours, sometimes longer
Also used to treating heroin withdrawal
Propoxyphene
By mouth-3 to 4 hours
Generally taken with aspirin or acetaminophen to
treat mild pain
Levorphanol
Intravenous or intramuscular-4 hours
By mouth-about 4 hours
Oral form is strong. Can be used instead of morphine
Hydromorphone
Intravenous or intramuscular-2 to 4 hours
By mouth-2 to 4 hours
Rectal suppository-4 hours
Begins wto work quickly. Can be used instead of
morphine. Helpful for cancer pain
Oxymorphone
Intravenous or intramuscular-3 to 4 hours
Rectal suppository-4 hours
Starts to work quickly
Oxycodone
By mouth-3 to 4 hours
Usually combined with aspirin or acetaminophen
Pentazocine
By mouth-up to 4 hours
Can block painkilling action of other opioids. About
as strong as codeine. Can cause confusion and
anxiety, especially for the elderly.
Source: The Merck Manual of Medical Infonnation Home Edition, Merck Research Laboratories, 1997
The Women, Suffer...
April Hazard Vallerand, Ph.D., R.N. , University of Pennsylvania School of Nursing in Philadelphia
(732.780.6224) reported the findings of a pilot study to assess the relationship of pain to functional status and
quality of life in women with HIV/AIDS. A sample of 25 women with HIV infection or AIDS with pain
complaints in a primary care clinic dedicated to the care of people with HIV were asked to complete several
assessment tools including the Brief Pain Inventory (BPI), the Inventory of Functional Status - Chronic Pain
(IFS-CP), the Functional Assessment of HIV Infection (FAHi) quality of life instrument, and a demographic
data sheet. The majority of participants had severe pain in the past week. Adequacy of analgesic therapy was
assessed using the Pain Management Index and the type and frequency of analgesics prescribed for pain.
Based on the PMI, 79% of the women reporting severe pain were receiving inadequate pain relief therapy. Of
the 12 participants reporting severe pain, 7 were receiving no analgesic therapy, while only 2 were prescribed
a strong opioid. The women with pain were found to have decreased functional status. Lower quality of life
scores were also found in those women with lower functional status.
Dr. Vallerand acknowledges in her conclusion a need for more information on the effects of pain and its
relationship to function status in women. But given previous data on the lack of effective pain medication
being offered to women, improving the management of pain in women should be a priority for clinicians.
Hospitalized Persons with AIDS). For this study, data
was gathered from audiotape, open-ended interviews
with eleven hospitalized people, film, literature, firstperson accounts and clinical observations. The
evaluative criteria of trustworthiness was applied to
assure rigor. The participants interviewed were a
mixed group: 8 men and 3 women, ages 28-44. Of
these 7 were white, 2 black, and 2 Latino. Eight
individuals had a history of chemical dependence
(either alcohol and/or cocaine and/or heroin).
From the interviews and other data five themes were
identified, four of which were common among all
participants: knowing pain, battling pain, pain's
influence and having AIDS. The fifth theme,
being a drug user, was found only among the
chemically dependent.
Theme 1 ("Knowing Pain") is focused on the difficult
task of describing pain and its impact on the body.
According to the study, participants often described
pain using metaphors, such as "It feels like someone
poking you with needles." Theme 2 (Battling Pain)
centers on the strategies adopted by individuals for
addressing pain and the barriers to pain relief.
Barriers include nurses, family members, friends and
patients themselves who do not take episodes of pain
seriously, especially among those with histories drug
addiction. Interestingly, Dr. Newshan reports that
participants both fought for and feared 'the big guns,'
or strong opiates. One participant described the
experience of opiates for pain management as "It's
like pulling teeth to get them" while another said the
morphine caused him/her "to feel like a zombie -- it
was scary." Under theme 3 (Pain's Influence) all of
the participants described the limitations placed on
their lives due to pain and, often, the greater
spirituality they gained.
Theme 4 (Having AIDS) related pain to the "uckky"
experience of having AIDS. And theme 5 (Being a
drug User) captures the very real experience of people
living with AIDS who have histories of drug use. For
these individuals pain management is made especially
hard because of the high tolerance to the effects of
opiates that their bodies have developed and the bias
of many healthcare providers in prescribing pain
medication to current or former drug users.
The participants of the study who all experience
multiple sources of pain which influences all of their
lives, and often feel unheard recommended the
following for clinicians:
I.
2.
3.
4.
5.
Listen to me.
Do not abandon me.
Keep trying.
Keep me informed.
Do not judge me.
Dr. Newshan concludes, "as healthcare givers, we
must ask [ourselves], 'Am I listening?"'
Duragesic: Another Route to Pain Relief
... While Drug Users Struggle
In a poster session Dr. Gayle Newshan, Ph.D., NP, St. Vincent's Hospital in New York City (212.604.7465)
reported on her study designed to increase understanding of the lived experience of pain in hospitalized people
with AIDS using a qualitative perspective (Is Anybody Listening? A Phenomenological Study of Pain in
Medical Alert • Issue One 1998
In another study conducted by Dr. Newshan with
Matthew Lefkowitz, MD, State University of New
York, Health Science Center at Brooklyn, New York
continued an page 11
3
(
Anyone can get HIV. Everyone should be
able to fight back.
Introducing VIRACEPT. A potent new protease inhibitor for children and adults.
The worrisome news is that women and children are
inhibitors. (The clinical significance of laboratory studies of
the fastest-growing groups becoming infected with HIV.
protease inhibitor resistance and changes in viral RNA
But now, treatments to combat the virus have shown
levels in blood has not been established for VIRACEPT.
promising results. VIRACEPT is a powerful new protease
The virus may still be present in other organ systems.)
inhibitor now available for the treatment of HIV infection
People treated with VI RACE PT may experience
in children (ages 2-13) and adults when anti-HIV drug
some side effects; the most common is diarrhea in
therapy is warranted.
approximately 200/o of people in clinical trials. There
VI RACE PT is available in tablets and a pleasant
are some common medications and some AIDS-related
tasting oral powder that can be mixed with water, formula,
medications you should not take with VIRACEPT. It
or dairy products. VIRACEPT is generally well-tolerated, is
is important to discuss with your doctor all other
taken three times a day with normal meals or light snacks,
medications that you or your child are taking.
and requires no special dietary restrictions.
We still can't make any long-term promises, since
Most importantly, VIRACEPT is effective. In many
it is not yet known whether taking VIRACEPT will help
adult patients, VIRACEPT lowered the amount of HIV in
you or your child live longer or reduce the number
the blood to levels below the limit of detection of the test
of infections or other illnesses that can occur with HIV.
used, and substantially increased CD4 cell counts after
But if you're ready to fight back, talk to your doctor
24 weeks of triple combination therapy. And in laboratory
about VIRACEPT. Or for more details, call toll free
studies, HIV obtained from five patients that became
1-888-VIRACEPT or visit www.agouron.com.
resistant to VI RACE PT was not resistant to other protease
VIRACEPT.
nelfinavir mesylate
Refer to the important information on the next page.
ff!l!!1f!!!'
Agouron_
Pharmaceuticals re
~
4
1997 Agouron Pharmaceuticals, Inc.
National Association of People with AIDS
(
5
Medical Alert • Issue one 1998
(
VIRACEPT
nelfi navi r rnesylate
Information for Patients About VIRACEPT" (Vl-ra-cept)
Generic Name: nelfinavir (nel-FIN-na-veer) mesylate
For the Treatment of Human Immunodeficiency Virus (HIV) Infection
Please read this information carefully before taking VIRACEPT. Also, please read this leaflet each time
rgruar~~~:;uttdif~~~~r~t~ttti~~~i:1loa;t~~1o~i~~l:6~rhd~~t~~- ~h~~I~
;i:~:~e~~ciPt:h:~~i~~t~~
zyl~~HW~ :~d;~~:~~ ~~fc~~~~geu!rs~~~~~~ft~Jgtuw1~~i~1 fr~:t!rki~~d!.\t~
ig~:
0JJcri~e
when taking
WHAT IS VIRACEPT AND HOW DOES IT WORK?
VIRACEPT is used in the treatment of people with human immunodeficiency virus (HIV) infection.
Infection with HIV leads to the destruction of CD4 T cells, which are important to the immune system.
After a large number of CD4 cells have been destroyed, the infected person develops acquired immune
desi1~li%¥~;~k~ebt~Po~king HIV protease (a protein-cutting enzyme), which is required for HIV to
multiply. VIRACEPT has been shown to significantly reduce the amount of HIV in the blood. You should
be aware, however, that the effect of VIRACEPT on HIV in the blood has not been correlated with longterm health benefits. Patients who took VIRACEPT also had significant increases in their CD4 cell count.
VIRACEPT Is usually taken together with other antlretrovlral drugs such as Retrovi,. (zidovudine,
AZT), Epivi,. ~lamivud1ne, 3TC), or Zerit" 15tavudine, d4T). Taking VIRACEPT in combination with other
ang~xiE~r m~~gg;;~~ec;tta~~Ws~~~~fes~~~:~. ~;li~rd\~~aJ 1e~i t~~~:i~~so~~:.
younger than 2 years of age are now taking place.
i~i~~. in infants
DOES VIRACEPT CURE HIV OR AIDS?
VIRACEPT is not a cure for HIV infection or AIDS. The long-term effects of VIRACEPT are not known at
~~i:o~ii~:d ~~~l~~kl~fec~l::ci~~em;r t~~~e dg~~~rio~~p~~u~~!ii~~~i~~ioh~~p~~ ~~~~~ fn°f~~~1~~ns~
Mycobacterium avium complex (MAC) infections, and Kaposi's sarcoma.
It is not known whether VIRACtPT will help you live longer or reduce the number of infections or other
illnesses that may occur..
There is no proof that VIRACEPT can reduce the risk of transmitting HIV to others through sexual
contact or blood contamination.
WHO SHOULD OR SHOULD NOT TAKE VIRACEPT?
yo:~gJ;~fs\:'.~:Oof~\1g~f~~';,~g~1~:edc~n~~c~~:thether VIRACEPT is appropriate for you. In making
Allergies: II you have had a serious alle111lc reaction to VIRACEPT, you must not take VIRACEPT.
You should also inform your doctor, nurse, or pharmacist of any known allergies to substances such as
ot~e;:ue~~;inper;;g~~t fh:s:ne~~~eit Zii~~.CSEPT on pregnant women or their unborn babies are not
known. If you are pregnant or plan to become pregnant, you should tell your doctor before taking
VIRACEPT.
II you are breast-feeding: You should discuss with your doctor the best way to feed your baby. You
should be aware that if your baby does not already have HIV, there is a chance that it can be transmitted
th~i~rdhr!~'.t~~~ii~"Pis~~~:~1:~g~l~."t~~:r~::-~~~~i\~:~~y2
3 years of age with HIV. There
is a powder form of VIRACEPT that can be mixed with milk, baby formula, or toads like pudding.
Instructions on how to take VIRACEPT powder can be found in a later section that discusses how
~~~~"~~vi
vi,~:~~~!v~rri~:~dl~~a~~~~ldR~'W,'f~~~dnot been studied in people with liver disease. If you have liver
disease, you should tell your doctor before taking VIRACEPT.
Other medical problems: Certain medical problems may affect the use of VIRACEPT. Be sure to tell
your doctor if you have hemophilia types A and B, diabetes mellitus, or an increase in thirst and/or
frequent urination.
CAN VIRACEPT BE TAKEN WITH OTHER MEDICATIONS?
VIRACEPT may interact with other drugs, including those you take without a prescription. You must
discuss with your doctor any drugs that you are taking or are planning to take before you take VIRACEPT.
Drugs you should nl!I take with VIRACEPT:
Seldane• (terfenadine, for allergies)
Hismana/9 (astemizole, for allergies)
Propulsid• (cisapride, for heartburn)
Cordarone•(amiodarone, for irregular heartbeat)
Quinidine (for irregular heartbeat), also known as Quinaglute~Cardioquin~Quinidex~and others
Ergot derivatives (Cafergot" and others, for migraine headache)
Halcion• (triazolam)
Versed" (midazolam)
Taking the above drugs with VIRACEPT may cause serious and/or life-threatening adverse events.
• Rifampin (for tuberculosis), also known as Rimactane•, Rifadin•, Rifater9, or Rifamate•
This drug reduces blood levels of VIRACEPT.
•
•
•
•
•
•
•
•
~~~~~~~~~l~~~euir~'.~:/IJ'tt)'.~~~
•
•
•
•
~~~~~:i!~~ a lower dose of Mycobutin.
A change ot therapy should be considered if you are taking VIRACEPT with:
Phenobarbital
Phenytoin (Dilantin• and others)
Carbamazepine (Tegretol• and others)
These agents may reduce the amount of VIRACEPT in your blood and make it less effective.
Oral contraceptives ("the pill")
U1~~;H~Tt~~~gr!~~g~ 1 ~~~ ~ff~~~i~~~~~~n;rgra1ycoounfr~~~~ti::. a different type of contraception since
HOW SHOULD VIRACEPT BE TAKEN WITH OTHER ANTI-HIV DRUGS?
Taking VIRACEPT together with other anti-HIV drugs increases their ability to fight the virus. It also
reduces the opportunity for resistant viruses to grow. Based on your history of taking other anti-HIV
medicine, your doctor will direct you on how to take VIRACEPT and other anti-HIV medicines. These
drugs should be taken in a certain order or at specific times. This will depend on how many times a day
each medicine should be taken. It will also depend on whether it should be taken with or without food.
Nucleoslde analogues: No drug interaction problems were seen when VIRACEPT was given with:
• Retrovir (zidovudine, AZT)
• Epivir (lamivudine, 3TC)
• Zerit,1.5tavudine, d4~
• ~i~~u ~~~d:an~~i;iot~ 1iidex (ddl) and VIRACEPT: Videx should be taken without food, on an empty
stomach. Therefore, you should take VIRACEPT with food one hour after or more than two hours before
you take Videx.
Nonnucleoside reverse transcriptase inhibitors (NNRTls):
When VIRACEPT is taken together with:
• Viramune• (nevirapine)
The amount of VIRACl:PT in your blood may be reduced. Studies are now taking place to learn about
• m~:~t~R~l~ombining VIRACEPT with Viramune.
VIRACEPT has not been studied with other NNRTls.
~~:~ ~~t:m+ni:it;:~~iogether with
6
• Crixivan• (indinavir)
The amount of both drugs in your blood may be increased. Currently, there are no safety and efficacy
data available from the use of this combination.
• Norvirr"" (ritonavir)
The amount of VIRACEPT in your blood may be increased. Currently, there are no safety and efficacy
data available from the use of this combinatmn.
• lnvirase• (saquinavir)
The amount of saquinavir in hour blood may be increased. If used in combination with saquinavir hard
~:~:ina~aJ:~\~!c~ ~~g ~v~~abi! ~~~:st~!i~Sen~f~~fse :i~;i~~fi~~- are needed. Currently, there are no
WHAT ARE THE SIDE EFFECTS OF VIRACEPT?
Like all medicines, VIRACEPT can cause side effects. Most of the side effects experienced with
VIRACEPT have been mild to moderate. Diarrhea is the most common side effect in people taking
~/~t~;.~i;;d2~$.s~f~~J[/n~~~~~~~f~gat:i~tr/1~d7~gr~;(tt\!~~;,F.~!)\~~;~nt~~~e;1~i~~!~ f6i~)";)
more loose stools a day. In most cases, diarrhea can be controlled using antidiarrheal medicines, such
~~:!te~~~t~i~![~~~~~,e~ni~
asci:~f
~t2e~~•:o~~~,3~!tf:~~~a~~~et:~g~l~~is~;ir~~~~de abdominal pain,
asthenia, nausea, flatulence, and rash.
There were other side effects noted in clinical studies that occurred in less than 2% of patients receiving
VIRACEPT. However, these side effects may have been due to other drugs that patients were taking or to
the illness itself. Except for diarrhea, there were not many differences in side effects in patients who took
VI RACE PT along with other drugs compared with those who took only the other drugs. For a complete list
of side effects, ask your doctor, nurse, or pharmacist.
HOW SHOULD I TAKE VIRACEPT?
ta~;~f;r~:1i~:i~ilg~~e smmm~6~1~c!?:::;~:cr1~~~:l~: 1~:!1b~~~ t~if~~~cV~~itJ;~~~~a~:
to~=~= 1
e::~!riye~~~:~~~-b~~g~~·/o0~octnotikri~~ f~;r~~~: 1 i~md~~~~:~ ~~~ d~s~a~~~he
number of doses per day. Also, take this medicine for the exact period of time that your doctor has
instructed. Do not stop taking VIRACEPT without flrsl consulllng wllh your doctor, even II you are
feeling better.
Only take medicine that has been prescribed specifically for you. Do not give VIRACEPT to others or
take medicine prescribed for someone else.
t1~ii;1
yo:~ed~~l~~~ ~~:it~:~:p;rWti b;/i~:r:~~!fr
~~~J~; ~nrtig~~li~0t~:v.;,~ii~ii::~n~~~~
somewhat consistent over time. Missing doses will cause the concentration of VIRACEPT to decrease;
therefore, you should not miss any doses. However, if you miss a dose, you should take the dose as
soon as possible and then take your next scheduled dose and future doses as originally scheduled.
fg~
~~:l~~6~~~~~e~n;~~~l~g;eh~1~1~lW~i 0/s~g~~nrih0/:."~blets) taken three times a day. Each
dose should be taken with a meal or light snack.
Pedlatl'lc Dose to Be Administered Three Times Dally
Number
of Level
Scoops•
Body Weight
Lb
Kg
8.5
10.5
12
14
16
18
to
to
to
to
to
lo
to
< 8.5
<10.5
<12
<14
<16
<18
<23
>23
15.5
18.5
23
26.5
31
35
39.5
<18.5
<23
<26.5
<31
<35
<39.5
to <50.5
>S0.5
Number
of Level
Teaspoons•
Number
of
Tablets
to
to
to
to
to
to
10
15
(n,~:::1u;~~go~r;6~t~~~e~Ot~gs~fVl~Am,sf'lf;e s:n~~lfh~~i~';,°~ provided with your VIRACEPT bottle.
' 1 level teaspoon contains 200 mg of VIRACEPT. Note: A measuring teaspoon used for dispensing
medlcallon should be used for measuring VIRACEPT Oral Powder. Ask your pharmacist to make sure
you have a medication dispensing teaspoon.
~~:ir~f~~w~~rA~:~i~r~\:,~w!i~~ ~e/~:~a:~~~nt of water, milk, formula, soy formula, soy milk,
dietary supplements, or dairy foods such as pudding or ice cream. Once mixed, the entire amount must
be taken to obtain the full dose.
Do not mix the powder with any acidic food or juice, such as orange or grapefruit juice, apple juice, or
1:f~~om temperature or refrigerated for up to 6 hours. Do
ap8~~!~~~epg!d~~~;
~:~1~:
not heat the mixed dose once it has been prepared.
Do not add water to bottles of oral powder.
VIRACEPT powder is supplied with a scoop for measuring. For help in determining the exact dose of
~:!e~~~
t~r~~
povi~Acf~Pf 0d!afht~W~~era~~~fa~Js°~~i~~~0~e~u;sl~i!c~~~~:!~!1tener, and therefore should not be
taken by children with phenylketonuria (PKU).
HOW SHOULD VIRACEPT BE STORED?
Keep VIRACEPT and all other medicines out of the reach of children. Keep bottle closed and store at
room temperature (between 59°F and 86°F) away from sources of moisture such as a sink or other damp
place. Heat and moisture may reduce the effectiveness of VIRACEPT.
Do not keep medicine that is out of date or that you no longer need. Be sure that if you throw any
medicine away, it is out of the reach of children.
Discuss all questions about your health with your doctor. If you have questions about VIRACEPT
ra~~Yvf~l!E~-r'm~inaX7.~2% \~\m.:sk your doctor, nurse, or pharmacist You can also call
Ef~~~?~~i:~
~e~lcfg~~~~gol~;y/~l~~~~rrit~ v~de~rf;t~)-~~et~egq~r~60~t~~~o:~~~:~~~~:~:~s~~~~~e
Inc; Seldane, Rifadin, Rifamate, Rifater/Hoechst Marion Roussel; Hismanal, Propulsid/Janssen
Pharmaceutica Inc; Halcion, Mycobutin/Pharmacia & Upjohn Co; Rimactane, Tegretol/CibaGeneva
Pharmaceuticals; Viramune/Roxane Laboratories, Inc: Oilantin/Parke-Oavis; Crixivan/Merck & Co, Inc;
8v~~i~
l~tig:~t~rf;£1~~~i~Q~~~i~ep~~oudeui~~~~~icckoi;:rb::Je~t1r.e~~b~~~°C~.0
Pharmaceuticals Corp. Norvir is a trademark of Abbott Laboratories.
l~6i g~;~~g~VN~
Issued 10/7/97
CALL 1.888. VIRACEPT
VIRACEPT is a registered trademark of Agouron Pharmaceuticals, Inc.
Ct997, Agouron Pharmaceuticals, Inc.
National Association of People with AIDS
•
--
Agota"011_
La Jolla, California, 92037, USA
(
Getting What You Need:
Annual Health Care
Access Guide
Produced with support from the U.S. Health Resources and Services Administration (HRSA)
Today, most people are aware of new treatment
strategies that work well for slowing or stopping
progression of illness in many people living with
HIV. Unfortunately, too many people Jiving with
HIV have not been able to take advantage of these
treatments because they do not have reliable access to
health care. As we learn more about HIV, we know
that getting into a coordinated system of care can be
critical to your survival.
While barriers to care remain, there are many
programs available to serve people living with HIV
and AIDS. Wherever you live, we urge you to
explore your health care options. The following
Health Care Access Guide is a starting point for
people living with HIV throughout the nation. We
urge you to use this guide to learn more about
programs that may be able to serve you. The Guide
provides basic information on federal health care
programs for which you may qualify. We also list
contact numbers to learn more about specific
program requirements. Most of these programs are
operated by state health departments, and some states
have additional programs that are not listed here.
If you have questions after reading this guide, we
invite you to call NAPWA's Health Education
Department for more information. Tina PerkinsGibson or Patrick Aiken will either answer your
questions or refer you to someone in your own state
or community who knows about specific programs
available in your area. An additional strategy
for learning about your health care options involves
contacting organizations in your community
that provide services for people living with HIV
and AIDS.
Studies have shown that persons diagnosed with HIV
infection and address their health care needs early,
are more likely to live healthier, and more productive
and fulfilling lives. To learn more about currently
recommended treatment strategies, contact I & R
Services for a copy of "Do You Know Your
Options?", a guide to antiretroviral therapy produced
by NAPWA to help you advocate for the best care.
Following are the programs that provide health
treatment access to people with HIV/AIDS.
Medicaid
Medicaid is a program operated by each state, where
the federal government pays at least half of the costs.
Approximately seventy percent of federal money
spent on health care for people living with HIV
comes through Medicaid. If you qualify, Medicaid,
either alone or with other programs listed here, is
probably your best option for getting into a
coordinated system of care. While the federal
government provides oversight and matching funds ,
each state's Medicaid program differs from others.
Medicaid provides mandatory services all states must
provide, and additional services that each state may
elect to provide. Services covered by all Medicaid
program include: hospital care, whether it is inpatient
(overnight stay) or outpatient (you return home the
same day you get health care services), doctor visits,
laboratory tests, x-rays, and nursing home and home
health services. Optional services may include
prescription drug benefits, clinic services, case
management services, and a range of other services.
In most cases, to qualify for Medicaid, adults with
HIV must be classified as disabled under the Social
Security Administration's definition. This generally
requires a person to have an AIDS diagnosis
(advocates are trying to expand Medicaid to cover
people living with HIV who do not have AIDS, but
this has not yet happened). Persons who meet the
Social Security criteria for disability and have an
income too high to qualify for Medicaid, may qualify
as "medically needy"--a special eligibility category
available in many states for persons who meet the
Medicaid income requirements after subtracting their
incurred medical expenses. Children living with HIV
and some mothers of children with HIV can qualify
for Medicaid if the family income is below a
certain level.
To determine if you qualify for Medicaid benefits,
contact the Medicaid program in your own state, at
the number listed below.
Medicare
Medicare is a national health insurance program that
provides health care security to America's seniors
and working people who have become disabled.
Medicare, unlike Medicaid, is administered solely
through the federal government.
Medicare has consisted of two parts. Part A provides
for hospital visits, and is financed through employee
and employer taxes. Part B provides supplementary
medical insurance, including doctor visits. This part
is funded through premiums paid by the individual
and general revenues. While Part B is voluntary,
most Part A enrollees participate in Part B. In the
Balanced Budget Act of I997, Congress created a
Part C called Medicare Plus Choice, which creates
more opportunities to enroll in managed care. For
people living with HIV, a major shortcoming of
Medicare is that it does not cover prescription drugs.
Many people with HIV in Medicare, however, are
also eligible for Medicaid, which they can use to
receive their drug benefits. Persons who are in both
Medicaid and Medicare are called dual-eligibles.
There are also two programs to help low-income
people cover costs of the Medicare program. The
Quality Medicare Beneficiary (QMB) and the
Medical Alert • Issue One 1998
Specified Low-Income Medicare Beneficiary
(SLMB) programs enable Medicaid to pay costsharing expenses and premiums for extremely lowincome Medicare recipients.
Medicare requires working age enrollees (under age
65) who become disabled (under the same disability
criteria as Medicaid) to have 40 quarters of
employment credit and be classified as disabled for
two years before they can receive benefits. To
determine if you are eligible for Medicare benefits,
including the QMB and SLMB Programs contact
your state representative listed below.
Ryan White CARE Act
The Ryan White CARE (Comprehensive AIDS
Resources Emergency) Act was enacted in 1990 and
reauthorized in 1996 to supplement Medicaid and
Medicare as our nation's response to the HIV
epidemic. Additionally, the CARE Act was intended
to provide assistance to cities that shouldered a
disproportionate number of AIDS cases, and to states
to build their infrastructures for responding to the
HIV epidemic. Named for the Indiana teenager who
was a hemophiliac with AIDS, the CARE Act is the
largest comprehensive program specifically for
people living with HIV. The CARE Act provides
health care services for low income, uninsured
and underinsured Americans who are either not
currently eligible for Medicaid or who do not have
private insurance.
The CARE Act charges the Federal government with
forming partnerships with state and local
governments, and community based programs and
AIDS service organizations, in order to provide care
and services to HIV infected persons. The CARE Act
is comprised of five Titles, each address ing a speci fic
component of HIV health care services.
Title I
Title I supports cities and metropolitan areas most
heavily impacted by HIV and AIDS. This title
provides emergency assistance for the delivery of
comprehensive HIV and AIDS medical care and
support services. Currently, nearly 49 metropolitan
areas receive Title I funding and support. Those
cities are listed in the state resource charts below.
Title II
Title II authorizes funds to every state, the District of
Columbia, Puerto Rico and other territories, to ensure
comprehensive and uniform services throughout the
nation. The services covered under thi s title include
prescription drugs, primary AIDS care services,
health care insurance continuation, and home health
care for persons living with HIV. These programs
are administered in urban , suburban and
rural communities.
7
Title II includes the AIDS Drug Assistance Program
(ADAP). Many HIV infected people receive HIV
drug therapies through their state's ADAP program.
Use the number listed for your state for more
information.
Title 111B
Title IIIB provides funding for community-base
clinics and public health providers to develop and
deliver early and ongoing comprehensive HIV/AIDS
services on an outpatient basis. Financial assistance
through this title services rural and underserved
urban areas, and particularly among women ,
adolescents and people of color.
Title IV
Title IV supports HIV services and clinical research
programs targeting populations for which the growth
rate of new infections is increasing rapidly, children,
youth, women and families. The majority of the
funds provide direct primary medical care. Contact
your state HIV/ AIDS office for information on
services offered in your area.
treatments for antiretrovirals and most opportunistic
infections. For more information of the programs,
and to determine if you are eligible, contact the
pharmaceutical companies listed below, or call
MedExpress at 1-800-808-8060 for assistance.
KEY CONTACTS
FOR
MORE INFORMATION
Colorado
AIDS Clinical Trials
AIDS clinical trails are studies conducted to help find
effective drug and other therapies for people living
with HIV. The treatments include experimental
antiretroviral and opportunistic infection drugs, and
alternative therapies. Clinical trials provide vital
information on new treatments. Participating in a
clinical trials is another way of taking positive action.
All drugs currently used have been studied through
clinical trials.
TIiie I
Connecticut
Title I
Delaware
Individuals living with HIV and health care providers
can find out more information on federally or
privately sponsored AIDS clinical trials by
contacting the Information Service listed below.
Eligibility requirements are different for each clinical
trial. Strict guidelines are used to protect patient
privacy and safety.
AIDS Office . . . . . . . . . . . .. (303) 692-2719
. ...... (303) 866-2993
Medicaid .
. .. 1-800-544-9181
Medicare .
... (303) 757-7227
Denver
Title 11/ADAP . .. . . . . . .. . . . (303) 866-2445
.... (860) 509-7832
AIDS Office
. .... (860) 424-5371
Medicaid .
. . 1-800--994-9422
Medicare.
........ (860) 527-0856
Hartford
New Haven .. . .......... (203) 392-6567
... 1-800-233-2503
Title 11/ADAP
AIDS Office.
Medicaid
Medicare
Title 11/ADAP ..
. ... (302) 739-3032
..... (302) 577-4900
.... 1-800-336-9500
. ........ (302) 739-3032
. (202) 727-2500
District of ColumbiaAIDS Office .
Medicaid .
. ... (202) 727-2500
Medicare ................ (202) 676-3900
Title I
... (202) 371-9100
Title 11/ADAP ............ (202) 727-2500
TitleV
Financial support from Title V funds are for the AIDS
Education and Training Centers (AETCs) and the
HIV/AIDS dental reimbursement programs. Also,
the Special Projects of National Significance (SPNS)
program is funded through this title. The AETC
program helps educate health care providers on
advances in HIV disease, to improve the delivery of
clinical care. The Dental program helps train dentists
to care for patients with HIV, and reimburses dental
schools who attend to the oral and dental needs of
indigent HIV infected patients.
AIDS Clinical Trials Information Service:
1-800-TRIALS-A (1-800-874-2572)
Title I
KEY CONTACTS
FOR
MORE INFORMATION
Georgia
Alabama
Veterans Benefits
Eligible veterans with HIV infection or AIDS may
receive a full range of services, ranging from testing
and counseling to acute and long-term care.
Eligibility for most VA benefits is based upon
discharge from active military service under other
than dishonorable conditions. The U.S. Department
of Veterans Affairs operates a system of health care
facilities throughout the United States. These
facilities include 172 medical centers, outpatient
clinics, Veterans Centers, nursing homes,
domiciliaries and or extended care programs such as
hospice care. To obtain a referral in your area call the
Veterans Benefits Number at 1-800-827-1000.
Drug Assistance Programs of
Pharmaceutical Companies
Many pharmaceutical companies have drug
assistance programs for people living with HIV who
are not able to afford medications. Each company
has eligibility criteria for their respective drug
8
AIDS Office
... (334) 206-5364
Medicaid
.... 1-800-362-1504
Medicare .
. .......... 1-800-243-5463
Title 11/ADAP .
. . (334) 206-5364
Alaska
AIDS Office ..
Medicaid.
Medicare
Title II/ADAP
American Samoa
Medicaid .
. ........ (648) 633-4590
Medicare .......... ..... 1-800-444-4606
Arizona
AIDS Office
...... (602) 230-5819
Medicaid ....... . .. .... . 1-800-962-6690
Medicare .
. ..... 1-800-432-4040
Phoenix .
. ........ (602) 277-7526
Title 11/ADAP
.... (602) 230-5819
Title I
..... (907) 269-8000
. ... (907) 465-3355
...... 1-800-478-6065
.... (907) 269-8058
Arkansas
AIDS Office .............. (501) 661-2135
Medicaid .
. .... (501) 682-6728
Medicare .
. .. 1-800-852-5494
Title 11/ADAP.
. ...... (501) 661-2292
California
AIDS Office.
. .. (916) 323-7415
Medicaid . .
. . (916) 445-0174
Medicare .
. .... 1-800-434-0222
Los Angeles ............. (213) 931-9828
Oakland/ Alameda Co ..... (510) 548-6511
Orange Co ....... ........ (714) 824-7758
Riverside/ San Bernadina ... (909) 387-6653
Sacramento. .
. ...... (916) 537-5353
San Diego .............. (619) 699-2514
San Francisco ............ (415) 554-9125
San Jose ................ (408) 258-2480
Santa Rosa/ Petaluma ..... (707) 869-2849
Title 11/ADAP .
. ..... (916) 327-6784
Other Resources
In addition to the federal health care programs listed
above, people infected with HIV may access
approved and experimental medications or medical
services through two other programs: Pharmaceutical
Company Drug Assistance Programs, and AIDS
Clinical Trials.
Florida
Title I
Title I
AIDS Office
........ (904) 487-3684
Medicaid .
. .. 1-850-488-3560
Medicare ............... 1-800-963-5337
Ft.Lauderdale/ Broward Co ... (954) 522-4749
Jacksonville _____________ (904) 630-1650
Miami / Dade Co. . ........ (305) 573-6010
Orlando.
. ......... (407) 862-4676
Tampa/ Saint Petersburg .... (813) 272-5040
West Palm Beach ......... (561) 833-2862
Title 11/ADAP .......... .. . (904) 413-0735
AIDS Office..
Medicaid
. .. (404) 657-3100
.... (404) 657-3590 or
1-800-869-1150
Medicare ............... 1-800-669-8387
Atlanta/Fulton Co .......... (404) 522-0400
Title 11/ADAP ............. (404) 657-3127
Guam
AIDS Office .............. (671) 734-7298
Medicaid.
. .... (671) 734-7269
Medicare .
. . 1-800-444-4606
...... (671) 734-7142
Title 11/ADAP
Hawaii
AIDS Office
Medicaid.
Oahu .
Other Islands
Medicare.
Title 11/ADAP .
Idaho
AIDS Office.
Medicaid.
. ..... (208) 334--6526
.... (208) 334-5747 or
(208) 334-5815
Medicare
... 1-800-247-4422
Title 11/ADAP ............. (208) 334-6526
Illinois
AIDS Office .
. . (312) 814-4846
Medicaid ............... 1- 800-252-8635
Medicare
.... 1-800-548-9034
Chicago.. .. . . . .. . .. . .. .. (773) 784-7297
Title 11/ADAP.
. .. 1-800-825-3518
Title I
.... (808) 733-9010
. ... (808) 587-3521
. ... (808) 587-3875
..... 800-518-8887
. . (808) 586-0100
. .. (808) 732-0026
Indiana
AIDS/Office .
. .. (317) 383-6867
Medicaid
_. (317) 232-4966
Medicare ............... 1-800-452-4800
Title 11/ADAP
.. (317) 920-3190
Iowa
. .... (515) 242-5838
AIDS Office.
Medicaid .
. ......... 1-800-972-2017
Medicare .
. ..... 1-800-351-4664
Title 11/ADAP .
. ..... (515) 242-5838
National Association of People with AIDS
continued on next page
(
I
KEY CONTACTS
FOR
MORE INFORMATION
'
AIDS Office
Medicaid.
Medicare
Title I1/ADAP ..
Kentucky
AIDS Office
..... (502) 564-6539
Medicaid . .
. .. 1-800-635-2570
Medicare ................ (502) 564-6539
Title I1/ADAP
..... (502) 564-6539
l
Louisiana
Title I
AIDS Office .
Medicaid.
Medicare.
Title II/AOAP .
... (207) 287-5551
..... (207) 287-3094
... 1-800-750-5353
.... (207) 287-5060
Maryland
AIDS Office.
Medicaid.
Medicare
Baltimore.
TI tie II/ADAP .
.. (410) 767-5013
....... (410)767-1432
... 1-800-243-3425
.... (410) 715-0895
. (410) 767-5087
Massachusetts
Title I
Michigan
TIiie I
Minnesota
TIiie I
Mississippi
Missouri
Title I
Montana
l
Nebraska
Nevada
New Hampshire
AIDS Office .
. ...... (603) 271-4576
Medicaid .. 1-800-852-3345 (x.4346 or 4344)
Medicare .
. 1-800-852-3388
Title 11/ADAP ...... 1-800-852-3345 (x4483)
Rhode Island
... (401 )277-2320
AIDS Office .
...... (401) 464-3361
Medicaid .
. 1-800-322-2880
Medicare ..
Title I1/ADAP . ..... (401) 222-2320 (x 107)
New Jersey
AIDS Office .
. ..... (609) 984-587 4
Medicaid .
. ...... (609) 588-2600
Medicare ............... 1-800-792-8820
Bergen/ Passaic .......... (201 I 523-8316
Hudson Co./ Jersey City. (201 I 795-4555x.26
Middlesex/ Somerset/
Hunterdon .
. ......... (908) 826-9160
Newark .
. . (201 I 483-4250
Vineland/ Millville/ Bridgeton (609) 825-6810
Title II/ADAP.
. .. (609) 984-6125
South Carolina
AIDS Office
Medicaid .
Medicare
Title II/ADAP .
South Dakota
AIDS Office .
. . (605) 773-3737
Medicaid .. (605) 773-3495 or (605) 945-5006
Medicare .
. ... 1-800-822-8804
Title I1/ADAP ............. (605) 773-3737
Tennessee
AIDS Office.
. . (615) 741-7500
Medicaid. 1-800-523-2863 or 1-800-669-1851
Medicare .. ............. 1-800-525-2816
TIiie I1/ADAP.
. . (615) 741 -8903
Texas
AIDS Office .
. ....... (512) 490-2515
Medicaid. 1-800-252-8263 or 1-800-252-9330
Medicare ............... 1-800-252-9240
Austin.
. .. (512) 450-1272
Dallas . . ............... (214) 368-0348
Fort Worth/ Arlington ...... (817) 921-7830
Houston .
. . (713) 526-8798
San Antonio.
. ... (210) 692-8831
Title I1/ADAP.
. . (512) 490-2510
Title I
..... (504) 586-7474
AIDS Office
. (504) 342-9240
Medicaid .
........... 1-800-259-5301
Medicare .
.... (504) 945-3229
New Orleans
..... (504) 568-7474
Title I1/ADAP .
Maine
Title I
J
..... (913) 296-6173
.... (913) 296-3349
... 1-800-860-5260
..... (913) 296-6036
Kansas
..... (617) 624-5300
AIDS Office
.. 1-800-841 -2900
Medicaid .
Medicare ............... 1-800-882-2003
Boston
.. (617) 498-1472
Title I1/ADAP ............. (617) 566-8358
AIDS Office .............. (517) 335-8468
Medicaid .
. 1-800-642-3195
Medicare ............... 1-800-803-7174
Detroit
.... (313) 864-8081
Title I1/ADAP .
. . (517) 335-9333
AIDS Office
.. (612) 623-5143
Medicaid.
. .... (612) 296-7675
Medicare ............... 1-800-333-2433
Minneapolis/ St. Paul ..... (612) 870-1723
Title I1/ADAP ............ (612) 297-3344
AIDS Office.
. . (601) 960-7711
Medicaid ................ (601 I 987-3944
Medicare
. 1-800-948-3090
Title I1/ADAP. .
. .. (601) 960-7723
..... (573) 751-6141
AIDS Office
Medicaid .
. 1-800-392-1261
Medicare .
... 1-800-390-3330
Kansas City
....... (816) 756-1304
St. Louis
....... (573) 658-1044
Title I1/ADAP . . . . . . . . . . . . (573) 751-6439
AIDS Office ..
. .... (406) 444-9028
Medicaid .. .. ............ (406) 444-4540
Medicare
... 1-800-322-2272
... (406) 444-4744
TIiie II/ADAP
AIDS Office ..
..... (308) 535-8134
Medicaid.
........ (402) 471-9147
Medicare. ............... (402) 471-2201
TI tie II/ADAP ............. (402) 559-4673
AIDS Office
Medicaid.
Medicare .
Title 11/ADAP
. (702) 687-4800
.... (702) 687-4776
. . 1-800-307-4444
....... (702) 687-4800
New Mexico
AIDS Office
.... (505) 476-8451
Medicaid ......... . ...... (505) 827-3100
Medicare ............... 1-800-432-2080
Title II/ADAP
....... (505) 476-8470
New York
AIDS Office
....... (518) 473-7542
Medicaid ................ (518) 486-9057
Medicare .
. .. 1-800-333-4114
New York City..
. (212) 869-3850
Dutchess Co .............. (914) 471-9185
Nassau/ Suffolk.
. .. (516) 968-3001
New York
...... (212) 788-2762
Title I1/ADAP ............. (518)459-1641
Title I
North Carolina
AIDS Office .. ........... (919) 715-3118
Medicaid .
. 1-800-662-7030
..... 1-800-443-9354
Medicare
.... (919) 715-3118
Title I1/ADAP
North Dakota
AIDS Office
Medicaid ..
Medicare .
Title II/ADAP .
Northern Mariana Islands
AIDS Office
Medicaid.
Medicare .
Ohio
Title I
. ... (701) 328-2378
.... 1101 I 328-2321
. 1-800-247-0560
.. 1101 I 328-2378
.... (614) 644-8026
AIDS Office
Medicaid.
....... (614) 466-6650
Medicare ............... 1-800-686-1578
Cleveland/ Lorain/ Elyria. .. (216) 664-4370
Title II/AOAP
........ (614) 466-6669
AIDS Office
.... (405) 271-4636
Medicaid ................ (405) 521-3679
Medicare ............... 1-800-763-2828
Title I1/ADAP
..... (405) 271-4636
Oregon
AIDS Office .............. (503) 731-4029
Medicaid. 1-800-273-0557 or 1-800-359-9517
Medicare .
. ....... 1-800-722-4134
Portland
.... (503) 248-5429
Title 11/ADAP
..... (503) 731-4029
Pennsylvania
Title I
Puerto Rico
Title I
AIDS Office . . . .......... (717) 783-0479
Medicaid . 1-800-692-7462 or (717) 787-3119
Medicare .
. 1-800-783-7067
Philadelphia
.. (215) 546-0300
Title I1/ADAP .
. ..... 1-800-922-9384
AIDS Office.
Medicaid .
Medicare.
Caguas .
Ponce
San Juan .
Title II/ADAP .
Utah
AIDS Office .............. (801 I 538-6096
Medicaid .
. ... 1-800-662-9651
Medicare
..... 1-800-439-3805
Title I1/ADAP .
. .. (801) 538-6096
Vermont
.... (802) 651-1533
AIDS Office
Medicaid .
..... 1-800-529-4060
Medicare ............... 1-800-642-5119
Title I1/ADAP .
. .... (802) 863-7245
Virginia
AIDS Office .............. (804) 786-6267
Medicaid .
. 1-804-692-1720
Medicare.
. . 1-800-552-3402
Title I1/ADAP . . .......... (804) 225-4844
Virgin Islands
AIDS Office ..
Medicaid
Medicare.
Title II/AOAP
........ (670) 234-8950
... (670-234-8950 x.2905
....... 1-800-444-4606
Oklahoma
Title I
Title I
.... (787) 274-5502
....... (809) 765-1230
........ (809) 721-8590
.......... (787) 745-0340
.... (787) 840-7510
. .. (787) 763-6560
.... (787) 763-4575
Medical Alert • Issue One 1998
..... (803) 737-4110
... (803) 737-5900
...... 1-800-868-9095
....... (803) 734-6033
. (809) 774-3168
. .... (809) 774-4624
. ..... (809) 774-2991
..... (809) 774-3168
Washington State AIDS Office .
. ......... (360) 586-8344
Medicaid ..
. .... 1-800-562-3022
Medicare .
. ... 1-800-397-4422
Title I
Seattle .
... (206) 720-4377
TI tie II/ADAP .
. . (360) 586-7388
West Virginia
AIDS Office.
.... (304) 558-5358
Medicaid .
. ... (304) 558-4098
Medicare . .
. ... 1-800-642-9004
Title II/ADAP ............. (304) 926-1758
Wisconsin
AIDS Office .
Medicaid .
Medicare
Title II/ADAP
Wyoming
AIDS Office .............. (307) 777-5932
Medicaid ................ (307) 777-7531
Medicare
.... 1-800-856-4398
Title I1/ADAP
..... (307) 777-5800
.. ... (608) 267-5287
. . 1-800-362-3002
.. 1-800-242-1060
...... (608) 267-6875
9
(
DRUG ASSISTANCE PROGRAMS OF
PHARMACEUTICAL COMPANIES
Acyclovir, Zovirax
Glaxo Wellcome Co............ . . 1-800-722-9294
Alpha lnterferon-2A, Roferon-A
Hoffmann-La Roche, Inc. . . . . . . . . . 1-800-443-6676
Alpha lnterferon-2B, lntron-A
Schering-Plough Corp.
. . 1-800-521-7157
Amitriptyline
Roche Laboratories . . .
. . 1-800-285-4484
Astemizole, Hismanal
Janssen Pharmaceutica . . . .
. ... 1-800-544-2987
Atovaquone, Meprone
Glaxo Wellcome Co.. . .
1-800-722-9294
Azithromycin, Zithromax
Pfizer, Inc.. . . . ................. 1-800-646-4455
A!J, Zidovudine Retrovir
Glaxo Wellcome Co...
1-800-722-9294
Bleomycin, Blenoxane
Brito I-Myers Squibb ..
. 1-800-272-4878
Cefitaxime, Claforan
Hoechst-Roussel ...
. 1-800-422-4779
Cehriaxone, Rocephin
Roche Laboratories ....
. 1-800-285-4484
Cefuroxime, Cehin
Eli Lilly and Company ..... . ........ 1-800-545-6962
Glaxo Wellcome.
. . 1-800-722-9294
Cimetidine, Tagamet
SmithKline Beecham ..
.... 1-800-546-0420
Ciproflaxacin, Cipro
Miles Pharmaceuticals.
.. 1-800-998-9180
Clarithomycin, Biaxin
Abbott Laboratories .
..... 1-800-688-9118
Clindamycin, Cleocine
Upjohn Company ...
... 1-800-242-7014
Clofazimine, Lamprene
Ciba Pharmaceuticals ....
.. 1-800-257-3273
Clonazepam, Klonopin
Roche Laboratories . .............. 1-800-285-4484
Clotrimazole, Mycelex,Lotrimin
Miles Inc
.................. 1-800-998-9180
Schering Laboratories . . . . .
. .. 1-800-656-9485
Cyclophosphamide, Cytoxan
Bristol-Myers Squibb ...
.. 1-800-272-4878
Cyclosporine, Sandimmune
Sandoz Pharmaceuticals ...
. . . . . . 1-800-631-8184
Daunorubicin, Lipsomal, DaunoXome
NeXstar Pharmaceuticals.
. .. 1-800-226-2056
ddC, Zalcitbane HIVID
Hoffmann-La Roche, Inc.
. 1-800-285-4484
Dexamethasone, Dacadron
Merck & Co. . .
. .... 1-800-994-2111
Didanosine, ddl, Videx
Bristol-Myers Squibb . . . .
. ... 1-800-272-4878
Dronabinol, Marinol
Roxane Laboratories. .
. ......... 1-800-274-8651
Doxcycline, Vibramycin
Pfizer Inc. .
. .. 1-800-646-4455
Doxorubicin, liposomal, Doxil
Sequus Pharmaceuticals
.. 1-800-375-1658
Erythropoietin, EPO, Procrit, Epogen
Ortho Biotech. .
. ......... 1-800-553-3851
Amgen..
. ..... 1-800-272-9376
Ethambutol, Myambutol
Wyeth-Ayerst. . . .
. .... 1-800-568-9938
10
Etoposide, VP16, Vepesid
Bristol-Myers Squibb . . . .
. ..... 1-800-272-4878
Erythromcyin
Wyeth-Ayerst. ................... 1-800-568-9938
Famciclovir, Famvir
SmithKline Beecham .............. 1-800-546-0420
Famotidine, Pepcid
Merck & Co ...................... 1-800-994-2111
Fentanyl, Duragesic
Janssen Pharmaceutica .. .......... 1-800-544-2987
Fluconazole, Diflucan
Pfizer, Inc .......... .
. 1-800-869-9979
Flucytosine, Ancobon
Roche Laboratories ..
.. 1-800-285-4484
Flucinonide, Lidex
Roche Laboratories . . . . . . . . . . . . . 1-800-285-4484
Fluoxetine hydrochloride, Prozac
Eli Lilly and Company.
. ... 1-800-545-6962
Foscarnet, Foscavir
Astra Pharmaceutical Products, Inc .... 1-800-488-3247
Ganciclovir, Cytovene
Roche Laboratories . . .
. . 1-800-285-4484
Ganciclovir, lntraocular, Vitrasert
Chiron Vision . . . . . . . . . . .
. 1-800-843-1137
G-CSF, Neupogen
Amgen ......................... 1-800-272-9376
GM-CSF, Leukine
lmmunex Corporation.
1-800-466-8639
Granisetron, Kytril
SmithKline Beecham ............ 1-800-866-6273
Hydrocortisone, Hydrocortone, Cortef
Merck & Co.. . . . . . .
. ... 1-800-994-2111
Upjohn Co..
. . 1-800-242-7014
Hydroxyzine, hydrochloride
Pfizer, Inc.
. .. 1-800-646-4455
Hydroxyzine pamoate,Vistaril
Pfizer, Inc.. . . . . . . . . . .
. 1-800-646-4455
Immune globulin, IV, WinRho SD
Univax.....
. .. 1-800-789-2099
lndinavir, Crixivan
. .... 1-800-927-8888
Merck & Co ....
ltraconazole, Sporanox
. ... 1-800-544-2987
Janssen Pharmaceutica .
Ketoconazole, Nizoral
Janssen Pharmaceutica .
... 1-800-544-2987
Lamivudine, 3TC, Epivir
Glaxo Wellcome Co ........... . .... 1-800-722-9294
Loperamide, lmodium
Janssen Pharmaceutica .
.... 1-800-544-2987
Laratadine, Claratin
Schering Laboratories ...
. .... 1-800-656-9485
Megestrol Acetate, Megace
. .. 1-800-272-4878
Bristol-Myers Squibb ...
Methotrexate, Rheumatrex
.. 1-800-568-9938
Wyeth Ayerst.
Methylprednisolone, Medrol
. 1-800-242-7014
Upjohn Co ..
Mexiletine, Mexitil
... 1-800-556-8317
Boehringer lngelheim.
Morphine sulfate, Roxanol
. . . 1-800-274-8651
Roxane Laboratories ...
Nizatidine, Axid
Eli Lilly and Co ......... .. .... .... 1-800-545-6962
Nystatin, Mycostatin
Bristol-Myers Squibb .............. 1-800-272-4878
Octreotide acetate, Sandostatin
Sandoz Pharmaceuticals ............ 1-800-631-8184
Oxandrolone, Oxandrin
Bio-Technology General Corp ........ 1-800-741-2698
Paclitaxel, Taxol
Bristol-Myers Squibb ....... .. ..... 1-800-272-4878
Paramomycin, Humatin
Parke-Davis . .
. .. 1-800-755-0120
Pentamidine aerosolized, NebuPent
Fujisawa Pharmaceuticals .......... 1-800-366-6323
Pentoxifulline, Trental
Hoechst Roussel Pharmaceuticals .... 1-800-422-4779
Phenytoin, Dilantin
Parke-Davis .....
. . 1-800-755-0120
Prednisone
... 1-800-656-9485
Schering Laboratories ..
Prochlorperazine, Compazine
SmithKline Beecham .....
. . 1-800-546-0420
Pyrazinamide, P.USP
Wyeth-Ayerst. . .
. .... 1-800-568-9938
Pyrimethamine, Daraprim, Fansidar
Glaxo Wellcome Co ....
. 1-800-722-9294
. 1-800-285-4484
Roche Laboratories
Ranitidine, Zantac
. 1-800-722-9294
Glaxo Wellcome ....
Rifabutin, Mycobutin
. . 1-800-366-5570
Pharmacia ..
Rifampin, Rimactane
. 1-800-257-3273
Ciba Pharmaceuticals.
Ritonavir, Norvir
. 1-800-659-9050
Abbott Laboratories .
Saquinavir, lnvirase
Roche Laboratories . .
. . 1-800-282-7780
Sertraline hydrochloride, Zoloh
Phizer, Inc. .
. ........ 1-800-646-4455
Stavudine, d4T
Bristol-Myers Squibb .
. .. 1-800-272-4878
Strptomycin, S.USP
Pfizer, Inc.. . . .
. . 1-800-254-4445
Sucralfate, Carafate
Marion Merrell Dow .
. .... 1-800-552-3656
Terfenadine, Seldane
Marion Merrell Dow .............. 1-800-552-3656
Testosterone, Transdermal patch
Alza Pharmaceuticals. .
. .... 1-800-634-8977
Trimethroprim sulfamethoxazole TMP/SMX,
Septra, Bactrim
. 1-800-722-9294
Glaxo Wellcome Co.... .
. . . . 1-800-285-4484
Hoffmann-La Roche .. .
Trimetrexate, Neu Trexin
. 1-800-285-4484
US Bioscience
Valacyclovir, Valtrex
.... 1-800-722-9294
Glaxo Wellcome .....
Vinblastine, Velban
... 1-800-545-6962
Eli Lilly and Company.
Vincristine, Oncovin
...... 1-800-545-6962
Eli Lilly and Company.
National Association of People with AIDS
(
Managing Pain
continued tram page 3
(718.625.4244) the authors compared the analgesic
efficacy of at least 15 days of a stable dose of oral
opoids with the analgesic efficacy of at least 15
consecutive days of therapy with fentanyl transdermal
system (Duragesic) in patients with AIDS related
chronic pain. Side effects, quality of life, and patient
satisfaction were also evaluated.
Fentanyl transdermal system (FfS) is delivered by a
noninvasive transdermal system (a skin patch) which
allows continuous delivery of a potent opioid
providing pain relief for up to 72 hours. While the
FfS is approved for the treatment of chronic pain in
people requiring opioid analgesia and research has
shown its effectiveness for treating cancer, the
product had not been evaluated for its effectiveness in
treating chronic pain in people with AIDS.
The study, supported by Janssen Research
Foundation, was an open-label, pre-treatment vs.
Post-treatment trial of outpatients at one site in the
United States. All patients had experienced at least
moderate pain control with a stable daily dose of a
potent oral opioid for the 3 days preceding
enrollment.
On enrollment (visit I), patients
completed a pain questionnaire and underwent a
history and physical examination. For 15 days,
participants remained on a stable dose of the oral
opioid analgesic that had been prescribed previously.
At The end of 15 days (visit 2) patients' medication
was titrated to a stable dose of FfS according to the
package insert instructions. After the participants had
received a stable dose of FfS for a least 15
consecutive days, the end of study (visit 3)
assessments were made. The assessments included
the Brief Pain Inventory before (visit 2) and after
(visit 3) 15 days of treatment with FfS.
Among the exclusion criteria were use of ritonavir
(Norvir) during the trial, life expectancy of less than
3 months, active substance abuse, and the inability to
speak, read or understand English.
A total of 35 individuals were enrolled in the study.
Of the group 74% were men, 26% were women; 37%
were Latino, 34% were black, 23% were white and
6% were of unknown racial origin. Nearly 70% of the
part1c1pants had completed high school, including
17% who had also completed college.
The
participants were divided among those who were
former intravenous drug users (43%), those who had
never used intravenous drugs (49%) and those who
were enrolled in a methadone treatment program
(8% ). At study start, most patients were taking more
than one medication for chronic pain: 71 % were
taking strong oral opioids and 45.7% were taking
nonsteroidal anti-inflammatory drugs, such as aspirin
or ibuprofen. Of those taking a strong opioid, the
majority (63%) were taking oxycodone plus
acetaminophen (Percocet) before beginning treatment
with the FfS.
The participants reported that the major impediments
to pain management were the difficulty of assessing
pain (74.3%), the belief that pain was part of their
condition (62.9%), and the fear of becoming addicted
to pain medication (54.3%).
The participants received therapy with FfS for a
mean of 22.5±1.9 days, and the mean dose
administered was 50±4.6mcg. During the FfS period, 32.4% of participants reported adverse events. The
most frequently reported side effects were headache, somnolence, and bronchitis, reported by 2 persons each.
Additionally, one participant died during
Figure 1
the oral opioid phase and one withdrew
Change in percent of pain relief by visit*
because of excessive somnolence during
the FfS phase.
100
The investigators report their study
shows Duragesic effectively alleviates
chronic pain in patients with AIDS . On
a scale of 0% to 100% relief, the mean :i
pain relief score increased from 77. I% ~
with oral opioids to 87.5% with FfS &
(figure 1). The Fentanyl transdermal
system provided an overall improvement
in general activity, mood, walking
ability, normal work, relationships, and
enjoyment of life over oral opioids
(figure 2). There was no difference in
adherence to therapy or frequency of
side effects in the two groups (figure 3).
80
c
60
40
20
0
Oral opioids
(Visit2)
Transdermal fentanyl
(Visit3)t
• A mean increase in score from visit 2 to visit 3 (visit 3 - visit 2 > 0)
indicates improvement. Item was scored as follows:
0%=no relief, to 100%=complete relief.
t P<0.001 (Wilcoxon's signed rand test).
Figure 2
Pain interference by type of activity*
Pain interferes 10
completely
9
LJ Transdermal fentanyI•
8
-
Oral opioids
7
6
5
4
3
2
Pain does
not interfere O General
activity
Mood
Walking Normal Personal
work relations
ability
Sleep Enjoyment
0 I118
fI
• P < 0.001 (Wilcoxn's signed rank test).
Figure 3
Satisfaction with pain medication
6
Ease
of use
Side effects
(frequency)
Side effects
(impact)
D
Transdermal fentanyl
-
Oral opioids
Delivery
mocte·
Met
expectations t
• P=0.03
t P=0.001 (Wilcoxon's signed rand test).
An informational brochure on pain in HIV/AIDS is available on NAPWAFax (Document No.1901)
at 202-789-2222. For additional information contact Cancer Care at 212-221-3300 or www.cancercareinc.org.
Medical Alert • Issue One 1998
11
FO
Added to
0
eatme
elines
Te
Panel on Clinical Practices in the Treatment of HIV
Infections, convened by the U.S. Department of Health
and Human Services and the Henry J. Kaiser Family
Foundation, has amended its guidelines to include
Fortovase (saquinavir), the new soft gelatin formulation
of the protease inhibitor Invirase (saquinavir mesylate)
manufactured by Hoffman-La Roche, among the list of
drugs in its preferred strategies. Fortovase was approved
for marketing by the FDA in November 1997 based in
part on data from study NV15355 which showed a
significantly greater proportion of patients, who received
Fortovase plus two nucleoside analogues, achieved viral
load reductions to below the limit of detection (400
copies/mL), as compared to those patients who have
received Invirase plus two nucleoside analogues at 16
weeks. Other studies considered in amending its
guidelines included NV15107, a dose ranging study, and
NV 15182, a safety study.
The guidelines were
formalized in November also and have been amended for
the first time following a review of data on the use of
Fortovase in clinical trials over 24 weeks.
Given at 1200 mg three times daily with meals, Fortovase
has been shown to provide increased level of drug to
attack HIV compared with Invirase. The primary side
effects are nausea, vomiting, diarrhea, flatulence,
abdominal discomfort and headaches. Tables 1 & 2 show
the percentage of people whose viral load levels were
below 400 copies/mL and 20 copies/mL after 6 months of
treatment in the Sun Study (M61005), an open label, noncomparative, two center study trial designed to evaluate
the efficacy of Fortovase in combination with two
nucleoside analogues. In the study, 42 treatment-naive
patients with more than 10,000 copies of HIV-RNNmL
of blood and CD4 counts greater than 100 cells received
Fortovase at 1200 mg three times daily, AZT at 300 mg
twice daily, and 3TC at 150 mg twice daily. Patients had
a mean baseline viral load of 65,757 copies and a mean
baseline CD4 count of 419 cells.
Hoffman-La Roche will continue to make Invirase
available to patients currently on the drug through early
summer. Following this period, patients who are
currently on Invirase will be able to receive the original
product under a limited distribution program. As always,
patients should discuss their future treatment options with
a knowledgeable physician.
12
SUN Study
FORTOVASE™ (SQV) SGC+AZT+3TC
% of Pts. with HIV-1 RNA< 20 COPIES/ml
80 ----------------------------------------(/)
t5
Q)
:0
70 ------------------------------------60
::J
en
0
50 ------------------------------
Q)
g'
c
Q)
~
40
30
Q)
a..
20 ---------------------10
0
2
4
6
8 12
Weeks
16
20
24
32
SUN Study
FORTOVASE™ (SQV) SGC+AZT+3TC
% of Pts. with HIV-1 RNA< 400 COPIES/ml
100~----------------(/)
~
80 ----------------------
:0
::J
en
0
Q)
Cl
ro
c
Q)
~
Q)
a..
20 -------
0
2
4
6
National Association of People with AIDS
8 12
Weeks
16
20
24
32
Niutnt1
( .. nNibbles
Body Composition Analysis
is an Important Tool
by Marcy Fenton, M.S., R.D. and
Stephanie Correnti, R.D.
Weight fluctuations measured on a scale may
not always be the truest indicator of changes in
lean body mass.
Bioelectric Impedance Analysis (BIA) is an
important tool to determine body composition.
Used in HIV-related wasting studies, BIA tests
are quick, accurate and relatively inexpensive
compared to some other body composition
tests. Along with viral load and CD4 count,
some physicians believe that BIA should be a
standard test for any HIV-infected person.
Body composition analysis provides early
detection of conditions so that changes can be
made at a time when they can be more effective
and less costly. These changes could involve
food, fluid, exercise or medications. It is a
powerful way to take control of your health.
Causes for weight loss and wasting
Usually, there are multiple reasons contributing
to the underlying mechanisms that cause weight
loss and wasting. The four main areas are:
• Lack of intake of calories and nutrientsreduced intake due to a decrease or loss of
appetite (anorexia), depression, illness, lack
of food, fatigue, nausea, vomiting, diarrhea.
• Malabsorption-vomiting, diarrhea, inability
to digest fats, lactose (the sugar that is found
in milk) or gluten (a protein found in
wheat flour).
• Metabolic changes-increased demand and
use of energy and protein. Hypogonadism,
which may originate as a result of weight
loss, is a decrease in the growth or functional
activity of the sexual organs, the testes or
ovaries, which then contributes to further
lean body mass losses.
• Reduction in use of muscle-from factors
such as illness, being fatigued, change in
lifestyle and depression.
Why test for body composition?
The BIA test should be performed soon after an
HIV diagnosis in order to establish a baseline.
Each person's result and progress is individual,
and each person acts as his/her own control.
The BIA test should be repeated at least two to
four times a year, and more depending on the
results of the previous tests, or changes in
nutritional or medical status.
Changes in body composition, specifically
changes in functioning tissue, should be
detected by performing a BIA test. Functioning
tissue-called body cell mass (BCM) and often
referred to as lean body mass (LBM)-is the
protein and active part of the cells found in
muscle and organs. BIA also identifies the
amounts of water in and outside the body cell
mass. Analysis of this fluid and fluid changes
can indicate an increase in muscle or wasting,
edema or dehydration. Most importantly,
changes in BCM and fluid can reflect positive
and negative changes in nutritional intake,
metabolism, response to disease and
effectiveness of treatment, so that outcomes
can be seen and interventions modified to be
made more effective.
To prepare for the BIA test, the following
guidelines should be observed:
• Do not exercise or use a sauna, steambath or
Jacuzzi eight hours or less prior to the test.
• Do not drink alcohol for 12 hours prior to
the test.
Do not be
or feverish."
tested
while
perspiring
• Do not skip any meals.
• Limit or eliminate caffeine-containing
beverages and food. Caffeine (found in
coffee, chocolate, colas, teas) is a
dehydrating agent that may affect the results
of the test.
• Although a specific amount of water intake
is not specified for the test, the usual
recommendation is to drink I0-12 cups of
fluid daily.
• Do not use diuretics, antihistamines or
steroids. Continue taking prescribed
Medical Alert • Issue One 1998
medication, but be prepared to tell v
drugs you are taking at the time of the te:
• An accurate weight and height is done at
time of testing.
• Prior to the test, remove jewelry on the
side of your body.
BIA Testing procedure:
The entire BIA test takes only five mim
to perform.
First, you will be asked to lay quietly with
motion flat on your back with arms and ii
separated away from the body so no parts .
touching or touching a wall. Using spec
adhesive pads, electrodes are attached on y<
right foot on the ankle and just below 1
middle toes, and on your right hand on the w1
and first joint of the middle finger.
To assure a better contact, areas of electro
placement will first be cleansed with rubbi
alcohol. (If you are sensitive to rubbi1
alcohol, let it be known to the pers1
administering the test.) The strength of t
electrical signal is very low. Most people do n
feel anything.
After the electrodes are removed, a qualific
health care professional should provide
opportunity to discuss the procedure with yo
either immediately following the test or at
follow-up appointment. Although the raw da
from the BIA test is available immediate!
complete analysis must be processed usin
special software.
When the test results have been processed,
copy will be sent to your physician.
If your doctor does not provide bod
composition testing, BIA tests are ofte
available at your local AIDS Services Provide
For more information, or for a referral to a
agency that provides BIA Testing, conta
NAPWA's Health Education Department.
I
Reprinted with permission from Positive Livin
Newsletter, December 1997. Marcy Fenton, M.S
R.D. is the HJV nutrition advocate at AJDS Proje
Los Angeles. Stephanie Correnti R.D., is t
registered dietitian at Project Angel Food.
13
(
HIV in Children
continued from page 1
5. Monitoring growth and development is important
for the care of HIV-infected children. Nutritional
support is a therapeutic intervention that affects
immune function, quality of life and bioactivity of
antiretroviral drugs.
6. Information regarding the efficacy of antiretroviral
drugs for children can be extrapolated from
clinical trials in adults. The absence of pediatricspecific clinical trials does not preclude the use of
any approved antiretroviral drug in children.
7 . Management of infants, children, and adolescents
with HIV/AIDS is
rapidly evolving and
increasingly complex, therefore, wherever
possible, management of HIV-infected children
and adolescents should be directed by a specialist
in the treatment of pediatric and adolescent HIV
infection. If this is not possible, then it is important
to consult with such experts regularly.
8. Adult guidelines for aniiretroviral therapy are
appropriate for adolescents.
Background information on HIV viral load:
The HIV RNA pattern among perinatal-infected
infants differs from that seen in infected adults. In one
large prospective study, HIV RNA levels were
generally low at birth (<I 0,000 copies/ml), rose to
extremely high values within the first 2 months of life
(most infants had values > 100,000 copies/ml), and
then fell very slowly; the mean HIV RNA level
during the first year of life was 185,000 copies/ml.
These very high levels only slowly decline over the
next few years of life to the set point value.
High RNA levels (above 100,000 copies/ml) in
infants have been shown to be associated with high
risk for disease progression and mortality, particularly
if the CD4+ lymphocyte percentage is under 15%. In
preliminary data from pediatric clinical trial, PACTG
152 correlating baseline virologic data with risk of
disease progression or death, there was a 54%
reduction in the relative risk of progression for each
log 1(10) decrease in baseline HIV RNA level.
Disease progression was documented in 11 % of
children 30 months old or less at entry (mean age, 1.1
years) with baseline RNA in the lowest quartile
(undetectable to 150,000 copies/ml) compared to
52% of those with baseline RNA in the highest
quartile (> 1,700,000 copies/ml). Among children
over 30 months old at entry (mean age, 7.3 years),
none of those with baseline RNA in the lowest
quartile (undetectable to 15,000 copies/ml) compared
to 34% of those in the highest quartile (> 150,000
copies/ml) had progression.
Key Recommendations
The Working Group recommendations for initiating
antiretroviral therapy in asymptomatic infants and
children with normal immune function are as follows :
Most Working Group participants would initiate antiretroviral
therapy in all HIV-infected infants under 12 months of age as
soon as a confirmed diagnosis is established regardless of
clinical status, immunologic status or viral load. HIVinfected infants under the age of twelve months are
considered at particularly high risk for disease
progression and the predictive value of immunologic
and virologic parameters to identify those who will
have rapid progression is Jess than at older ages.
Most Working Group members also favored the approach of
initiating therapy in all HIV infected children older than 12
months regardless of age or symptom status in order to treat
infected children as early as possible in the course of disease
and intervene prior to immunologic deterioration.
Alternatively, some Working Group members would defer
treatment in asymptomatic children and would carefully
monitor clinical, immunologic and virologic status. In such
cases, factors that should be considered in deciding to initiate
therapy include: development of clinical symptoms; rapidly
declining CD + lymphocyte number or percentage to values
approaching the moderate immune suppression threshold; and ,
high or increasing HIV RNA levels. Although the level of
RNA considered indicative of increased risk for disease
progression is not well defined in young children Jess
than 30 months of age, the Working groups concluded
that RNA level >100,000 copies/ml is clearly
indicative of a high risk for mortality. For those
children over 30 months of age, most Working Group
members would also initiate treatment at lower HIV
RNA levels (e.g. greater than 15,000 to 20,000), more
consistent with the adult guidelines.
2. Choice of Antiretroviral Therapy:
Combination therapy is recommended for all infants,
children and adolescents who are treated with antiretroviral
agents. When compared to monotherapy, combination
therapy: 1) slows disease progression and improves
survival, 2) results in a greater and more sustained
virologic response, and 3) delays development of
resistant mutations.
Most Working Group participants recommend aggressive
antiretroviral therapy for primary prenatal infection with 3
drugs, believing that this approach provides the best
opportunity to delay progression and possibly to eradicate
HIV infection. Based on clinical trials in infected adults,
the preferred regimen to accomplish this is
combination therapy with two nucleoside analog
reverse transcriptase inhibitors (NRT!s) and one
protease inhibitor (see table 3).
continued an next page
Table 2
1994 Revised HIV Pediatric Classification System:
Clinical Categories
CATEGORY N: NOT SYMPTOMATIC
Children who have no signs or symptoms considered to be the result of HIV infection or who have only ONE of the conditions
listed in Category A.
CATEGORY A: MILDLY SYMPTOMATIC
Children with TWO or more of the conditions listed below but none of the conditions listed in categories B and C.
• Lymphadenopathy (>0.5 cm at more than two sites; bilateral + one site)
• Hepatomegaly
• Splenomegaly
• Dermatitis
• Parotitis
• Recurrent or persistent upper respiratory infection, sinusitis or otitis media
CATEGORY B: MODERATELY SYMPTOMATIC
Children who have symptomatic conditions other than those listed for Category A or C that are attributed to HIV infection.
Examples of conditions in clinical category B include but are not limited to:
• Anemia (<8 gm/dl), neutropenia (<1,000/mm_), or thrombocytopenia (<100,000/mm_) persisting® 30 days
• Bacterial meningitis, pneumonia, or sepsis (single episode)
• Candidiasis, oropharyngeal (thrush) persisting (> 2 months) in children > 6 months of age
• Cardiomyopathy
• Cytomegalovirus infection, with onset before 1 month of age
• Diarrhea, recurrent or chronic
• Hepatitis
• Herpes simplex virus (HSV) stomatitis, recurrent (more than two episodes within 1 year)
• HSV bronchitis, pneumonitis, or esophagitis with onset before one month of age
• Herpes zoster (shingles) involving at least two distinct episodes or more than one dermatome
• Leiomyosarcoma
• Lymphoid interstitial pneumonia (LIP) or pulmonary lymphoid hyperplasia complex
• Nephropathy
• Nocardiosis
• Persistent fever (lasting > 1 month)
• Toxoplasmosis, onset before 1 month of age
• Varicella, disseminated (complicated chickenpox)
1. When to Initiate Antiretroviral Therapy:
CATEGORY C: SEVERELY SYMPTOMATIC
Antiretroviral therapy is recommended for all HIV infected
infants and children with clinical symptoms of HIV infection
(CDC Clinical Category A, B or Cl or evidence of immune
suppression (CDC Immune Category 2 or 3), regardless of
viral load.
14
Children who have any condition listed in the 1987 surveillance case definition for acquired immunodeficiency
syndrome, with exception of LIP (which is category B condition)
Modified from: Centers for Disease Control. 1994 Revised Classification System for Human Immunodeficiency Virus
in Children Less than 13 Years of Age. MMWR 1994;43 (No. RR-12): 1-10
National Association of People with AIDS
(
Table 3
Recommended Antiretroviral
Options for Initial Therapy of
Pediatric HIV Infection
While Working Group participants favor an initial approach
to therapy with two NRTls and a protease inhibitor, it is
recognized that some may favor a more conservative
approach and would initiate therapy with 2 NRTls,
particularly if there were concerns by the caregiver
regarding the feasibility of carrying out a complex threedrug regimen or the patient and family preferred a 2-drug
regimen. Alternative regimens have shown clinical
Preferred Regimen: Evidence of clinical benefit and
sustained suppression of HIV RNA in clinical trials in infected
adults; studies in pediatric patients are ongoing.
One highly active protease inhibitor plus 2 NRTls
• Protease inhibitor: *
Preferred protease inhibitor for young children:
Ne/finavir
benefit in adult and pediatric patients, although these
regimens may not suppress viral load to below
detectable levels as does combination therapy with 2
NRTis and a protease inhibitor. Such alternative
regimens include combination regimens of two
NRTis alone or combination therapy of two NRTis
with a non-nucleoside reverse transcriptase inhibitor,
substituted for the protease inhibitor.
Alternatives
Ritonavir
lndinavir !for children who can swallow pills)
• Recommended dual NRTI combinations:
Most data in children:
ZDV + ddl
ZDV + 3TCt
More limited data in children:
3. When to Consider Changing Antiretroviral Therapy:
d4T + ddl
D4T + 3TCt
There are 3 main reasons for considering changing
antiretroviral therapy:
ZDV + ddCtt
Failure of the current regimen with evidence of
disease progression based on either clinical, virologic
or immunologic parameters; 2) toxicity or
intolerance to the current regimen; 3) new data
demonstrating that a drug or regimen is superior to
the current regimen.
Alternative Regimens: Less likely to produce sustained
HIV RNA suppression in infected adults; combination
nevirapine, ZDV and ddl produced dramatic and sustained
viral suppression in two of six infants first treated at< 4
months of age in small preliminary pediatric study.
(Luzuriaga 97)
Nevirapine + 2 NRTls (as above)
or
3 NRTls: d4T + ddl + 3TC
Clinical disease progression includes: I) progressive
neurodevelopmental deterioration; 2) growth failure
defined as persistent decline in weight growth
velocity despite adequate nutritional support and
without further explanation; 3) disease progression,
as defined by advancement from one CDC Clinical
category to another.
Secondary Alternative Regimen: Clinical benefit
demonstrated in clinical trials in infected adults and/or
children, but initial viral suppression may not be sustained.
2 NRTls (one of the recommended dual NRTI
combinations listed above)
Immunologic disease progression includes: I)
progression from one CDC Immune Category to
another; 2) a persistent decline of 5 percentiles or
more in those with < 15% CD4 + lymphocytes; and
3) rapid and extensive decrease within a given CDC
immunologic category.
Not Recommended: Evidence against use due to
overlapping toxicity and/or virologically undesirable
Any monotherapy
d4T + ZDV
ddC + ddl
ddC + d4T
ddC + 3TC
Special Issues with Adherence for
HIV Infected Children & Adolescents
Lack of adherence to prescribed regimens and
subtherapeutic levels of antiretroviral medications
may enhance the development of drug resistance,
particularly to protease inhibitors. Therefore,
education of the child or adolescent and/or his/her
caregivers regarding the importance of compliance
with the prescribed drug regimen is necessary at the
time of initiation of therapy, with continued
reinforcement at subsequent visits.
Infants and young children are dependent upon
others for administration of medication; thus ,
assessment of the capacity for adherence to a
complex multi-drug regimen requires evaluation of
the caregiver and his or her environment as well as
the ability and willingness of the child to take the
drug. Liquid formulations or formulations suitable
for mixing with formula or food are necessary for
administration of oral drugs to young children.
Lack of palatability of such formulations may
be problematic if the child is to accept and retain
the medication.
For adolescents, treatment regimens must balance the
goal of prescribing a maximally potent antiretroviral
regimen with realistic assessment of existing and
potential supports to facilitate adherence. In order to
meet the multiple needs of HIV infected adolescents,
who are frequently unexperienced with health care
systems, comprehensive systems of care are required
to serve both medical and psychosocial needs.
Coordinated, comprehensive, family-centered
systems of care can often address many of the day-today problems facing children, adolescents, and
families that may affect their adherence to complex
medical regimens. Case managers, mental health
counselors, peer educators, outreach workers
and other members of the multidisciplinary team
may often be able to address specific barriers
to adherence.
I@
NAP WA wishes to thank the National Pediatric and Family HIV Resource Center and the New Jersey
AIDS Education and Training Center (S. Grubman, MD, J. Oleske, MD, G. Scott, MD, L. Mofenson, MD, and
C. Burr, RN, MS) for their assistance.
Please see the guidelines for important notes on
these therapeutic options.
~~
someol7e you
dune 27th
NATIONAL HIV
TESTING DAY
J
U
N
E
2
TAl(J:~~1
7
Medical Alert • Issue One 1998
15
:>a 'uo:a,6U!4SBM
MN ':a,aaJ:a.S >I £Lt L
Ztt£-SOOOZ
Medical Alert is a free, health education newsletter. To ensure you receive each
issue, please complete and return this coupon .
Free subscriptions are made possible through the generous support of our Friends.
Please help us continue our health education work by making a tax-deductible
contribution of $25 or more to support Medical Alert and NAPWA's important work.
Information contained in this
publication is for educational
purposes only and does not
constitute an endorsement.
Copyright © 1998 NAPWA
Permission to duplicate is
granted and encouraged provided
the source is acknowledged.
Name
Organization (if applicable)
Editor
Charles Nelson
Street Address
Managing Editor
Matthew Doerpinghaus
City/ State / Zip
Phone
FAX
Email
How can we better serve you?
0
I want to support the important health education and advocacy work of
NAPWA. Enclosed is my tax-deductible gift to NAPWA's Circle of Friends.
Mail, FAX or Email to:
NAPWA. 1413 K Street NW.
Washington DC 20005-3442
FAX: 202-898-0435 , Email : medical_alert@napwa.org
Contributors
Patrick Aiken
C. Burr, RN, MS
Stephanie Correnti, R.D.
Jeffrey S. Crowley, M.P.H.
Anthony Farmer, M.B.A.
Marcy Fenton, M.S., R.D.
S. Grubman, MD
L. Mofenson, MD
J. Oleske, MD
G. Scott, MD
Executive Director
A. Cornelius Baker
world wide web
www.napwa .org
2 Intense:
Mark Ameen
The Buried Body
Dennis Cooper
Idols
Amethyst Press
author's
John Gilgun
OutWrite '91 Music I Never Dreamed OJ
reading.
Bo Houston
Horse and Other Stories
Remember Me
Kevin Killian
Bedrooms Have Windows
Stan Leventhal
The Black Marble Pool
Patrick Moore
This Every Night
David Trinidad
Hand Over Heart
Saturday
March 2nd
4 pm - 6pm
Cathedral Hill Hotel
Japanese Pavilion
(800) 331-4427
Cash Bar
Call For A Free Brochure
The newest information source on gay and
lesbian relationships ... an absolute must...order
today-risk free trial offer!
YES! Please send me COUPLES at the special
introductory rate of $25.50 for 12 issues (15%
savings of the regular rate). If I am not delighted
with the first issue, I will simply write "cancel" on
your bill and return it without owing a thing.
Name _ _ _ _ _ _ _ _ _ _ _ __
Address _ _ _ _ _ _ _ _ _ _ _ __
City/ST/Zip _ _ _ _ _ _ _ _ _ __
_ Check enclosed for $25.50
ai
~
o
RESIST
We've been funding peace and
social justice for 23 years;
some recent grants include:
Abortion Rights Fund of Western Mass. (Hadley, MA);
ACT UP/LA (CA); Concord Feminist Health
Center (NH); Gay & Lesbian Resource Center (Des
Moines, IA); Gay Community News (Boston, MA);
Lambda Rights Network (Milwaukee, WI); National
Latina/o Lesbian & Gay Organization (Washington, DC);
Puerto Rican Women's Committee (Boston, MA);
Southeastern Conference for Lesbians & Gay Men '90
(Raleigh, NC); Texas Lesbian Conference (San Antonio,
TX); and The Women's Project (Little Rock, AR).
For information, grant guidelines, or to make a
donation (and receive our newsletter), write to:
RESIST, Box OL, One Summer Street,
Somerville, MA 02143
617-623-5110
Funding Social Change Since 1967
_ Bill-me
TWT Press, Inc., P.O. Box 155, Boston, MA 02124
or Fax 617-287-8361
THE 12TH INTERNATIONAL
CONFERENCE OF
GAY AND LESBIAN JEWS
Son Francisco, California • Moy 24-27, 1991
Join gay, lesbian and bisexual Jews
throughout the world for afun, spiritual,
informative and exciting weekend conference.
Registration fees
For attendees from
United States or Canada
Other notions
untn March I 5 alter March I 5
$135
$110
$160
$135
The registration fee includes: one lunch; one
dinner dance; one brunch; lesbian/gay
comedy and music show; Shabbat services
and oneg shabbat; four workshop sessions;
keynote speaker; and much more.
Send your
check or write
to us for more
information:
12th International Conference
c/o Congregation Sha'ar Zahav
220 Danvers Street
Son Francisco, California 94114
USA
Telephone 1415) 861-6932
Part of Medical Alert : no.1(1998)